

372 |
|
Week 8: Fluids |
|
|
|
|
|
|
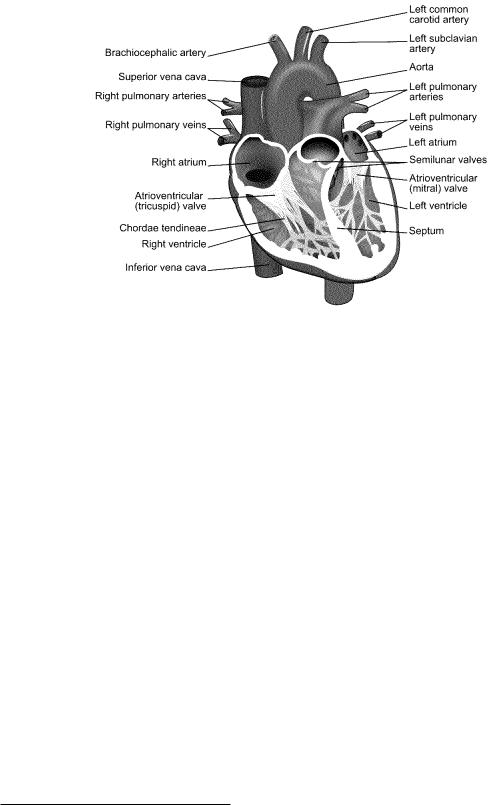
Figure 115: A simple cut-away diagram of the human heart.
8.5: The Human Circulatory System
For once, this is a chapter that math majors, physics majors, and engineers may, if they wish, skip, although personally I think that any intellectually curious person would want to learn all sorts of things that sooner or later will impact on their own health and life. To put that rather bluntly, kids, sure now you’re all young and healthy and everything, but in thirty or forty more years (if you survive) you won’t be, and understanding the things taught in this chapter will be extremely useful to you then, if not now as you choose a lifestyle and diet that might get you through to then in reasonably good cardiovascular shape!
Here is a list of True Facts about the human cardiovascular system, in no particular order, that you should now be able to understand at least qualitatively and conceptually if not quantitatively.
•The heart, illustrated in the schematic in figure 115 above162 is the “pump” that drives blood through your blood vessels.
•The blood vessels are di erentiated into three distinct types:
–Arteries, which lead strictly away from the heart and which contain a muscular layer that elastically dilates and contracts the arteries in a synchronous way to help carry the surging waves of blood. This acts as a “shock absorber” and hence reduces the peak systolic blood pressure (see below). As people age, this muscular tissue becomes less elastic – “hardening of the arteries” – as collagen repair mechanisms degrade or plaque (see below) is deposited and systolic blood pressure often increases as a result.
159The argument won’t quite be identical – the potential di erence V there will relate to current more like the way F does to flow in our treatment, rather than P , so electrical resistance will be inversely proportional to A, not A2.
160Wikipedia: http://www.wikipedia.org/wiki/Reynolds Number.
161Wikipedia: http://www.wikipedia.org/wiki/hydraulic diameter.
162Wikipedia: http://www.wikipedia.org/wiki/Human heart. The diagram itself is borrowed from the wikipedia
creative commons, and of course you can learn a lot more of the anatomy and function of the heart and circulation by reading the wikipedia articles on the heart and following links.
Week 8: Fluids |
373 |
Arteries split up the farther one is from the heart, eventually becoming arterioles, the very small arteries that actually split o into capillaries.
–Capillaries, which are a dense network of very fine vessels (often only a single cell thick) that deliver oxygenated blood throughout all living tissue so that the oxygen can disassociate from the carrying hemoglobin molecules and di use into the surrounding cells in systemic circulation, or permit the oxygenation of blood in pulmonary circulation.
–Veins, which lead strictly back to the heart from the capillaries. Veins also have a muscle layer that expand or contract to aid in thermoregulation and regulation of blood pressure as one lies down or stands up. Veins also provide “capacitance” to the circulatory system and store the body’s “spare” blood; 60% of the body’s total blood supply is usually in the veins at any one time. Most of the veins, especially long vertical veins, are equipped with one-way venous valves every 4-9 cm that prevent backflow and pooling in the lower body during e.g. diastoli (see below).
Blood from the capillaries is collected first in venules (the return-side equivalent of arterioles) and then into veins proper.
•There are two distinct circulatory systems in humans (and in the rest of the mammals and birds):
–Systemic circulation, where oxygenated blood enters the heart via pulmonary veins from the lungs and is pumped at high pressure into systemic arteries that deliver it through the capillaries and (deoxygenated) back via systemic veins to the heart.
–Pulmonary circulation, where deoxgenated blood that has returned from the system circulation is pumped into pulmonary arteries that deliver it to the lungs, where it is oxygenated and returned to the heart by means of pulmonary veins. These two distinct circulations do not mix and together, form a closed double circulation loop.
•The heart is the pump that serves both systemic and pulmonary circulation. Blood enters into the atria and is expelled into the two circulatory system from the ventricles. Systemic circulation enters from the pulmonary veins into the left atrium, is pumped into the left ventricle through the one-way mitral valve, which then pumps the blood at high pressure into the systemic arteries via the aorta through the one-way aortic valve. It is eventually returned by the systemic veins (the superior and inferior vena cava) to the right atrium, pumped into the right ventricle through the one-way tricuspid valve, and then pumped at high pressure into the pulmonary artery for delivery to the lungs.
The human heart (as well as the hearts of birds and mammals in general) is thus fourchambered – two atria and two ventricles. The total resistance of the systemic circulation is generally larger than that of the pulmonary circulation and hence systemic arterial blood pressure must be higher than pulmonary arterial blood pressure in order to maintain the same flow. The left ventricle (primary systemic pump) is thus typically composed of thicker and stronger muscle tissue than the right ventricle. Certain reptiles also have four-chambered hearts, but their pulmonary and systemic circulations are not completely distinct and it is thought that their hearts became four-chambered by a di erent evolutionary pathway.
•Blood pressure is generally measured and reported in terms of two numbers:
–Systolic blood pressure. This is the peak/maximum arterial pressure in the wave pulse generated that drives systemic circulation. It is measured in the (brachial artery of the) arm, where it is supposed to be a reasonably accurate reflection of peak aortic pressure just outside of the heart, where, sadly, it cannot easily be directly measured without resorting to invasive methods that are, in fact, used e.g. during surgery.
–Diastolic blood pressure. This is the trough/minimum arterial pressure in the wave pulse of systemic circulation.

374 |
Week 8: Fluids |
Blood pressure has historically been measured in millimeters of mercury, in part because until fairly recently a sphygnomometer built using an integrated mercury barometer was by far the most accurate way to measure blood pressure, and it still extremely widely used in situations where high precision is required. Recall that 760 mmHg (torr) is 1 atm or 101325 Pa.
“Normal” Systolic systemic blood pressure can fairly accurately be estimated on the basis of the distance between the heart and the feet; a distance on the order of 1.5 meters leads to a pressure di erence of around 0.15 atm or 120 mmHg.
Blood is driven through the relatively high resistance of the capillaries by the di erence in arterial pressure and venous pressure. The venous system is entirely a low pressure return; its peak pressure is typically order of 0.008 bar (6 mmHg). This can be understood and predicted by the mean distance between valves in the venous system – the pressure di erence between one valve and another (say) 8 cm higher is approximately ρbg × 0.08 ≈= 0.008 bar. However, this pressure is not really static – it varies with the delayed pressure wave that causes blood to surge its way up, down, or sideways through the veins on its way back to the atria of the heart.
This di erence in pressure means one very important thing. If you puncture or sever a vein, blood runs out relatively slowly and is fairly easily staunched, as it is driven by a pressure only a small bit higher than atmospheric pressure. Think of being able to easily plug a small leak in a glass of water (where the fluid height is likely very close to 8-10 cm) by putting your finger over the hole. When blood is drawn, a vein in e.g. your arm is typically tapped, and afterwards the hole almost immediately seals well enough with a simple clot su cient to hold in the venous pressure.
If you puncture an artery, on the other hand, especially a large artery that still has close to the full systolic/diastolic pressure within it, blood spurts out of it driven by considerable pressure, the pressure one might see at the bottom of a barrel or a back yard swimming pool. Not so easy to stop it with light pressure from a finger, or seal up with a clot! It is proportionately more di cult to stop arterial bleeding and one can lose considerable blood volume in a very short time, leading to a fatal hypotension. Of course if one severs a large artery or vein (so that clotting has no chance to work) this is a very bad thing, but in general always worse for arteries than for veins, all other things being equal.
An exception of sorts is found in the jugular vein (returning from the brain). It has no valves because it is, after all, downhill from the brain back to the heart! As a consequence of this a human who is inverted (suspended by their feet, standing on their head) experiences a variety of circulatory problems in their head. Blood pools in the head, neck and brain until blood pressure there (increased by distension of the blood vessels) is enough to lift the blood back up to the heart without the help of valves, increasing venous return pressure in the brain itself by a factor of 2 to 4. This higher pressure is transmitted back throughout the brain’s vasculature, and, if sustained, can easily cause aneurisms or ruptures of blood vessels (see below)) and death from blood clots or stroke. It can also cause permanent blindness as circulation through the eyes is impaired163
Note, however, that blood is pushed through the systemic and pulmonary circulation in waves
163
”You are old, Father William,” the young man said, ”And your hair has become very white;
And yet you incessantly stand on your Do you think, at your age, it is right?”
”In my youth,” Father William replied to his son, ”I feared it might injure the brain;
But now that I’m perfectly sure I have none, Why, I do it again and again.”
Not really that good an idea...
