


216 Part V – Biliary Tree Abnormalities
101Hilar Cholangiocarcinoma IV – Metal Stent with Interval Growth
Most patients with hilar cholangiocarcinoma (CC) clinically present with painless jaundice; however, other common symptoms include pruritus, weight loss, and abdominal pain. Although surgical resection offers the only hope for cure, most patients are found to have unresectable disease on initial presentation and have an extremely grim prognosis. This has led to an emphasis on the role of palliative care, with relief of biliary obstruction, in the management of these patients. Surgery of cholangiocarcinoma has been replaced by percutaneous biliary stent placement. After several months, stents may become occluded by debris or tumor growth. MR imaging can reliably demonstrate tumor growth in the presence of the stent.
MR Imaging Findings
At MR imaging, stent causes susceptibility artifacts mainly on the gradient echo sequences. Despite these artifacts, the tumor detection and delineation is very reliable at MR imaging. The tumor as well as any liver metastases have moderately high signal compared to the liver. The lesions show irregular rim enhancement with transient wedge-shaped enhancement in the arterial phase. In the delayed phase, parts of the tumor show persistent enhancement. On MRCP sequences, the increase in the distance between the right and the left biliary system indicates indirect interval tumor growth (Figs. 101.1 – 101.3).
Literature
1.Lee MJ, Dawson SL, Mueller PR, et al. (1993) Percutaneous management of hilar biliary malignancies with metallic endoprostheses: results, technical problems, and causes of failure. Radiographics 13:1249 – 1263
2.Hanninen EL, Pech M, Jonas S, et al. (2005) Magnetic resonance imaging including magnetic resonance cholangiopancreatography for tumor localization and therapy planning in malignant hilar obstructions. Acta Radiol 46:462 – 70
3.Freeman ML, Oyerby C (2003) Selective MRCP and CT-targeted drainage of malignant hilar biliary obstruction with self-expanding metallic stents. Gastrointest Endosc 58:41 – 9
4.Reinhold C, Bret PM (1996) Current status of MR cholangiopancreatography. AJR 166:1285 – 1295
5.Inal M, Akgul E, Aksungur E, et al. (2003) Percutaneous self-expandable uncovered metallic stents in malignant biliary obstruction. Complications, follow-up and reintervention in 154 patients. Acta Radiol 44: 139 – 146
Management
Reobstruction is the most common late complication after stent placement for hilar CC. In such cases, reintervention should be considered.
101 Hilar Cholangiocarcinoma IV – Metal Stent with Interval Growth 217
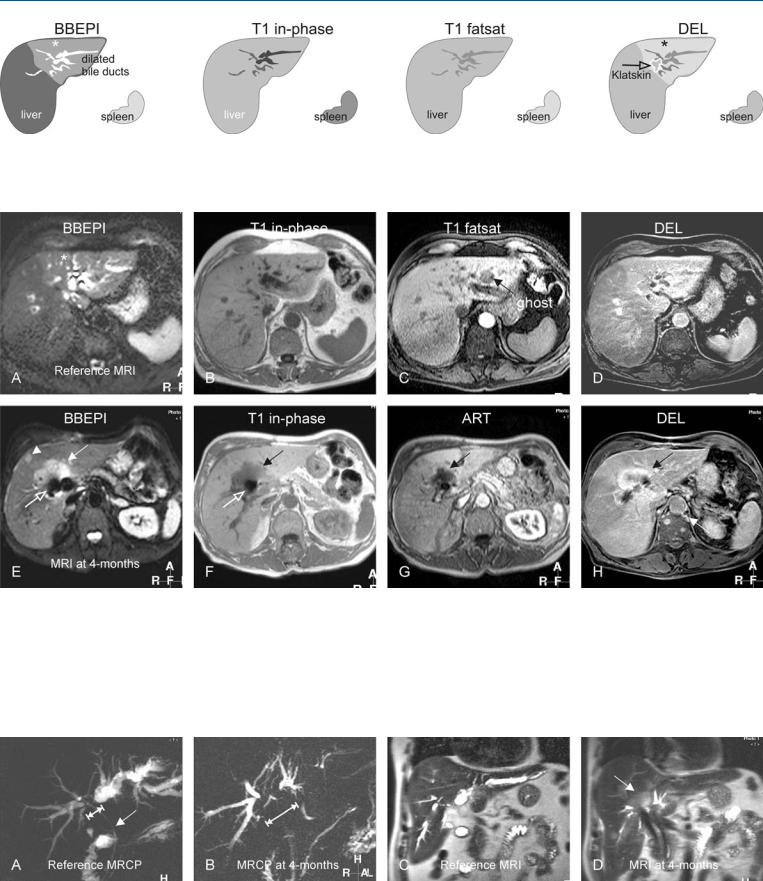
Fig. 101.1. Hilar cholangiocarcinoma, drawings. BBEPI: dilated left-sided bile ducts surrounded by edema (*); no mass is visible; T1 in-phase: pneumobilia rendering dark signal within bile ducts after placement of an endopros-
Fig. 101.2. Hilar cholangiocarcinoma (CC), interval growth, MRI findings. A Axial TSE image (T2 fatsat): Dilated left-sided bile ducts with edema (*); no mass is visible. B Axial in-phase image (T1 in-phase): Status post endoprosthesis with pneumobilia rendering some of the bile ducts very dark. C Axial GRE image (T1 fatsat): No mass is visible. D Axial delayed phase image (DEL): CC is slightly less enhanced than the surrounding liver. Note also slightly increased parenchymal enhancement. E Axial TSE image (T2 fatsat) at 4 months follow-up shows considerable increase in the hilar mass (solid
thesis; T1 fatsat: no mass is visible; DEL: Klatskin tumor is slightly less enhanced than the surrounding liver. Note also the slightly increased parenchymal enhancement (*)
arrow) that appears hyperintense to the liver with encasement of the metallic stent (open arrow), placed after removal of the endoprosthesis. Note also a metastasis (arrowhead). F Axial in-phase image (T1 in-phase): note the stent (open arrow) in the center of the mass (solid arrow). G Axial arterial phase image (ART) shows heterogeneous enhancement. H Axial delayed phase image (DEL): CC is better delineated from the surrounding liver (arrow)
Fig. 101.3. Hilar cholangiocarcinoma, interval growth, MRCP versus MRI findings. A MRCP shows mainly the dilated bile ducts in the left liver with a plastic stent in situ (arrow) with indirect suggestion of a hilar mass (double arrow).
B MRCP (at 4 months) suggests an increased size of the hilar mass (doubleheaded arrow). C Coronal SSTSE image shows dilated bile ducts. D Coronal SSTSE image at 4 months shows the hilar mass (arrow)
218 Part V – Biliary Tree Abnormalities
102Hilar Cholangiocarcinoma V – Biliary Dilatation Mimicking Klatskin Tumor at CT
The appearance of most liver lesions is well established at imaging. However, considerable overlap may be present among the appearance of various lesions. Computed tomography (CT) is well known for the occurrence of pseudolesions and pitfalls. Particularly, some cystic lesions may contain fluid with higher density than simple fluid and mimic solid lesions. Most CT examinations are performed as single (portal) phase contrast-enhanced examinations, and lack the dynamic enhancement pattern information which might facilitate distinction between benign and malignant lesions. In addition, the low intrinsic soft tissue contrast does not allow distinction between high fluid-content and solid liver lesions.
Literature
1.Ito K, Honjo K, Fujita T, et al. (1996) Liver neoplasms: diagnostic pitfalls in cross-sectional imaging. Radiographics 16:273 – 293
2.Yoshimitsu K, Honda H, Kuroiwa T, et al. (2001) Unusual hemodynamics and pseudolesions of the noncirrhotic liver at CT. Radiographics 21:S81– S96
3.Hanninen EL, Pech M, Jonas S, et al. (2005) Magnetic resonance imaging including magnetic resonance cholangiopancreatography for tumor localization and therapy planning in malignant hilar obstructions. Acta Radiol 46:462 – 70
4.Reinhold C, Bret PM (1996) Current status of MR cholangiopancreatography. AJR 166:1285 – 1295
MR Imaging Findings
At MR imaging, lesions or structures with high fluid content, such as dilated bile ducts, display very high signal intensity on heavily T2-weighted sequences and hence allow easy distinction from solid lesions. In addition, many centers perform routine dynamic gado- linium-enhanced imaging, which provides additional information concerning the benign versus malignant nature of the lesions. Therefore, cystic dilatation of the bile ducts which may mimic a solid lesion at CT can be correctly identified as a benign lesion at MR imaging (Figs. 102.1 – 102.3).
Management
MR imaging may prevent unnecessary surgery and can be used for follow-up of lesions causing pitfalls at CT.
102 Hilar Cholangiocarcinoma V – Biliary Dilatation Mimicking Klatskin Tumor at CT 219
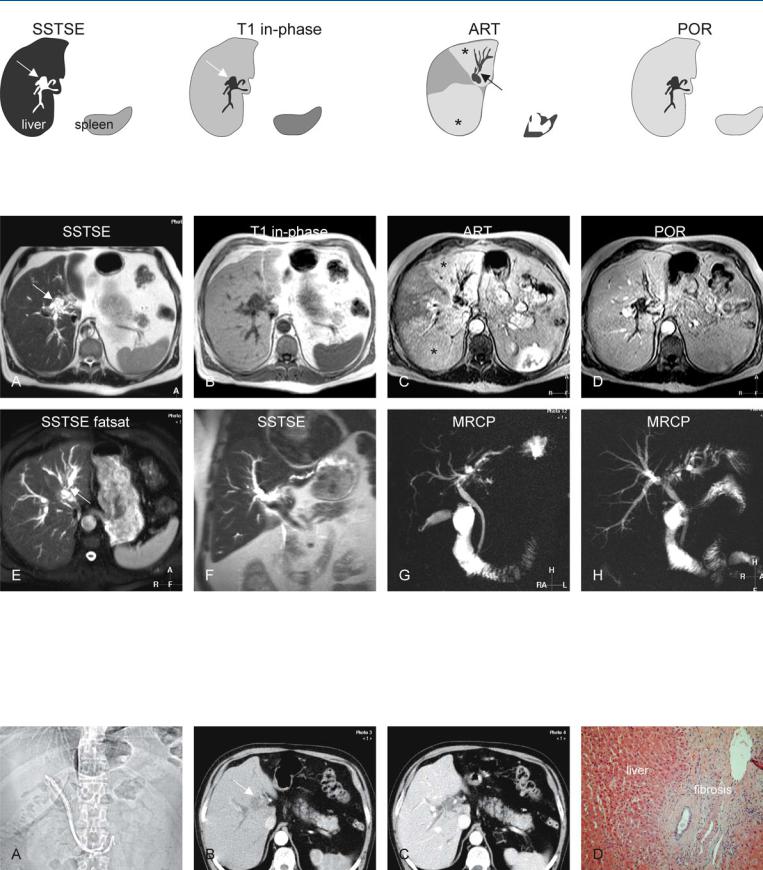
Fig. 102.1. Biliary dilatation mimicking cholangiocarcinoma at CT, drawings.
SSTSE: local fusiform dilatation of the bile ducts (arrow), without a mass. T1 in-phase: dilated bile ducts (arrow); ART (slightly different anatomic level):
Fig. 102.2. Biliary dilatation mimicking cholangiocarcinoma at CT, MR findings. A Axial SSTSE image (SSTSE): dilated bile ducts without a mass (arrow). B Axial in-phase image (T1 in-phase): Dilated bile ducts are hypointense (arrow). C Axial arterial phase image (ART): Wedge-shaped enhancement
(*) suggests compression of the bile ducts and/or cholangitis. D Axial portal phase image (POR): The liver parenchyma surrounding the dilated bile ducts shows homogeneous enhancement. E Axial fat-suppressed SSTSE im-
wedge-shaped areas suggest biliary compression or cholangitis (*). Note a local biliary stenosis (arrow); POR: homogeneous enhancement of the liver surrounding the dilated bile ducts
age (SSTSE fatsat) at a different anatomic level shows dilated bile ducts as well as a stenosis (arrow); no mass is seen. F Coronal SSTSE image (SSTSE): Again dilated bile ducts are present on both sides of the liver. G A 2D 40-mm- thick-slab MRCP (MRCP) shows the dilated intrahepatic bile ducts as well as the common bile duct. H MRCP from another angle provides an overview of the abnormal bile ducts. Based on MR imaging, CT diagnosis of CC was questioned; subsequent biopsies were negative for malignancy
Fig. 102.3. Biliary dilatation mimicking cholangiocarcinoma at CT. A Scout view shows the endoprosthesis in-situ. B CT in the arterial phase: One of the dilated bile ducts was mistaken for a hilar mass (arrow). C CT in the portal phase shows homogeneous enhancement of the liver. D Photomicrograph
taken from one of the several biopsies performed after MRI shows fibrosis and normal liver tissue without any evidence for malignancy. H&E stain, × 100