


104 Part IIC – Primary Solid Liver Lesions in Cirrhotic Liver
49HCC in Cirrhosis VIII – Segmental Diffuse with Portal Vein Thrombosis
Diffuse hepatocellular carcinoma (HCC) is present in 4 – 13 % of patients with HCC. The tumor can spread throughout most of the liver, and may be segmental in location. Typically, diffuse HCC is accompanied by extensive portal venous tumor thrombosis and a substantial elevation of serum alpha-fetoprotein (AFP) value. Serum AFP values may be elevated in up to 78 % of patients. Diffuse HCC is often difficult to detect on imaging studies because of its permeative appearance and heterogeneity of background chronic liver disease. Portal venous tumor thrombosis may be an important clue to the diagnosis. Fibrous capsule and septa are often absent in diffuse HCC. Detection of portal venous thrombosis is crucial in the diagnosis of diffuse HCC on imaging.
Literature
1.Kanematsu M, Semelka RC, Leonardou P, et al. (2003) Hepatocellular carcinoma of diffuse type: MR imaging findings and clinical manifestations. JMRI 18:189 – 195
2.Okuda K, Noguchi T, Kubo Y, et al. (1981) A clinical and pathological study of diffuse type hepatocellular carcinoma. Liver 1:280 – 289
3.Tublin ME, Dodd 3rd GD, Baron RL (1997) Benign and malignant portal vein thrombosis: differentiation by CT characteristics. AJR 168:719 – 723
4.Kelekis NL, Semelka RC, Worawattanakul S, et al. (1998) Hepatocellular carcinoma in North America: a multiinstitutional study of appearance on T1-weighted, T2-weighted, and serial gadolinium-enhanced gradi- ent-echo images. AJR 170:1005 – 13
MR Imaging Findings
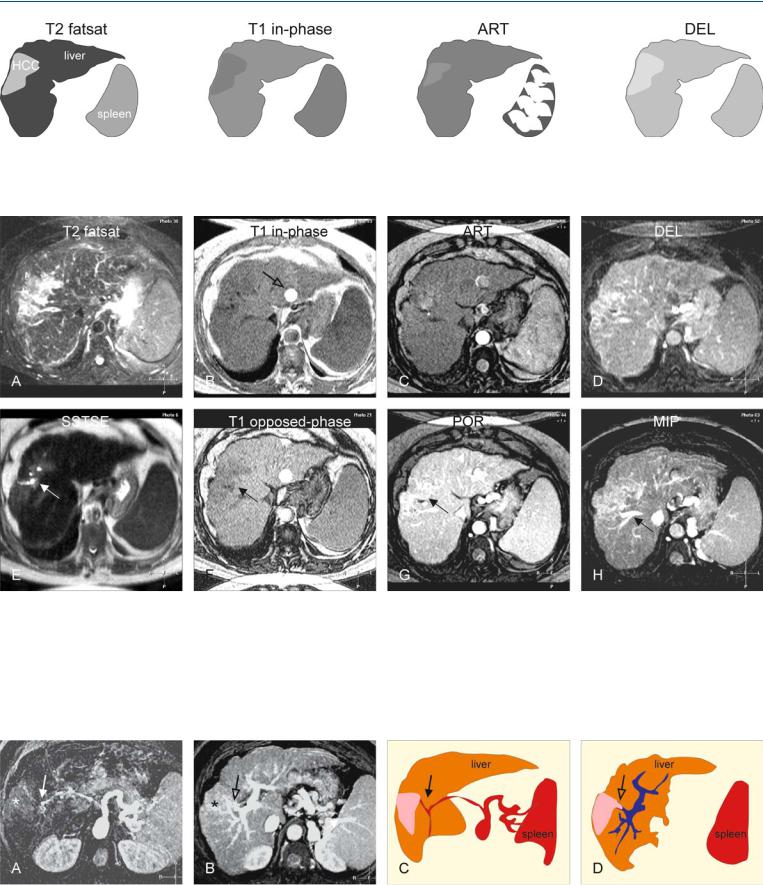
At MR imaging, the affected segment(s) have subtle to markedly increased signal intensity on T2-weighted images. On heavily T2weighted images, segmental dilatation of the bile ducts may also be present. On T1-weighted images, subtle hypointensity may be present. On gadolinium-enhanced images, the affected area may show only faint heterogeneous or patchy enhancement in the arterial phase. However, the lesion may show markedly heterogeneous enhancement in the delayed phase, likely due to a combined effect of washout and ongoing persistent enhancement (Figs. 49.1, 49.2). In some cases, portal vein thrombosis may be masked by the presence of the tumor. If necessary, maximum intensity projections may facilitate evaluation of the extent of the portal vein thrombosis (Fig. 49.3). Ascites may surround the liver. Hepatic veins are often unaffected.
Differential Diagnosis
Confluent fibrosis may be a challenge to distinguish from diffuse HCC on CT. MR imaging provides more characteristic imaging information.
49 HCC in Cirrhosis VIII – Segmental Diffuse with Portal Vein Thrombosis 105
Fig. 49.1. HCC, cirrhotic diffuse HCC, portal invasion, iron deposition. T2 fatsat: HCC is much brighter than the dark liver due to mild iron deposition; the spleen has also a lower signal; T1 in-phase: HCC is slightly hypointense to
Fig. 49.2. HCC, cirrhotic liver, diffuse HCC, portal invasion, iron deposition, MRI findings. A Axial fat-suppressed TSE image (T2 fatsat): HCC is much brighter than the dark liver and the spleen due to iron deposition. B Axial in-phase GRE image (T1 opposed-phase): HCC is slightly hypointense compared to a slightly darker liver and spleen [liver and spleen have become darker compared to opposed-phase (shorter TE) image in F]. Pulsation artifact of the aorta (open arrow). C Axial arterial phase image (ART): HCC shows faint heterogeneous enhancement. D Axial delayed phase image (DEL): HCC
the cirrhotic liver (irregular contours and splenomegaly); ART: a part of HCC shows faint heterogeneous enhancement; DEL: HCC shows some washout and becomes more heterogeneous
shows some washout and becomes more heterogeneous. E Axial SSTSE image (SSTSE): HCC contains dilated bile ducts (arrow).The liver and the spleen are too dark due to iron deposition. F Axial opposed-phase image (T1 opposed-phase): HCC (arrow) is more hypointense in a brighter liver due to shorter TE. G Axial portal phase image (POR): HCC appears somewhat heterogeneous (arrow). H Maximum intensity projection (MIP): HCC shows no invasion of the right hepatic vein (arrow)
Fig. 49.3. HCC, diffuse in cirrhosis with portal invasion, MIPs and drawings. A A MIP of the arterial phase: The hypertrophic hepatic artery (solid arrow) feeds the tumor (*). B MIP of the portal phase: Note the disruption of the portal branch to segment VIII (open arrow), due to invasion (*). C Drawing
shows the hypertrophic hepatic artery caused by the presence of cirrhosis and HCC (solid arrow). D Drawing illustrates the tumor invasion of the portal branch to segment VIII (open arrow)

106 Part IIC – Primary Solid Liver Lesions in Cirrhotic Liver
50 HCC in Cirrhosis IX – Multiple Lesions Growing on Follow-up
In a large multi-institutional study of 354 hepatocellular carcinomas (HCCs), 56 % were solitary, 40 % multiple and 4 % diffuse. Multiplicity of HCC may be based on transhepatic hematogenous spread, multifocal origin, or a combination of both. In general, the differential diagnosis of hypervascular liver lesions is wide-rang- ing. However, in the setting of cirrhosis the differential diagnosis can be practically narrowed down to HCC unless proven otherwise. Therefore, it is crucial to know the patient’s history (e.g., viral and alpha-fetoprotein status) and to determine any morphological changes that suggest fibrosis or cirrhosis on imaging. These include
(1) irregular or rounded liver contours; (2) abnormally large or small liver segments; (3) presence of nodules; (4) splenomegaly; (5) collaterals; and (6) ascites. Recognition of cirrhosis is particularly important if a patient presents with multiple hypervascular lesions.
Literature
1.Kelekis NL, Semelka RC, Worawattanakul S, et al. (1998) Hepatocellular carcinoma in North America: a multiinstitutional study of appearance on T1-weighted, T2-weighted, and serial gadolinium-enhanced gradi- ent-echo images. AJR 170:1005 – 1013
2.Ito K, Fujita T, Shimizu A, et al. (2004) Multiarterial phase dynamic MRI of small early enhancing hepatic lesions in cirrhosis or chronic hepatitis: differentiating between hypervascular hepatocellular carcinomas and pseudolesions. AJR 183:699 – 705
3.Hussain SM, Zondervan PE, et al. (2002) Benign versus malignant hepatic nodules: MR imaging findings with pathologic correlation. Radiographics 22:1023 – 1036
MR Imaging Findings
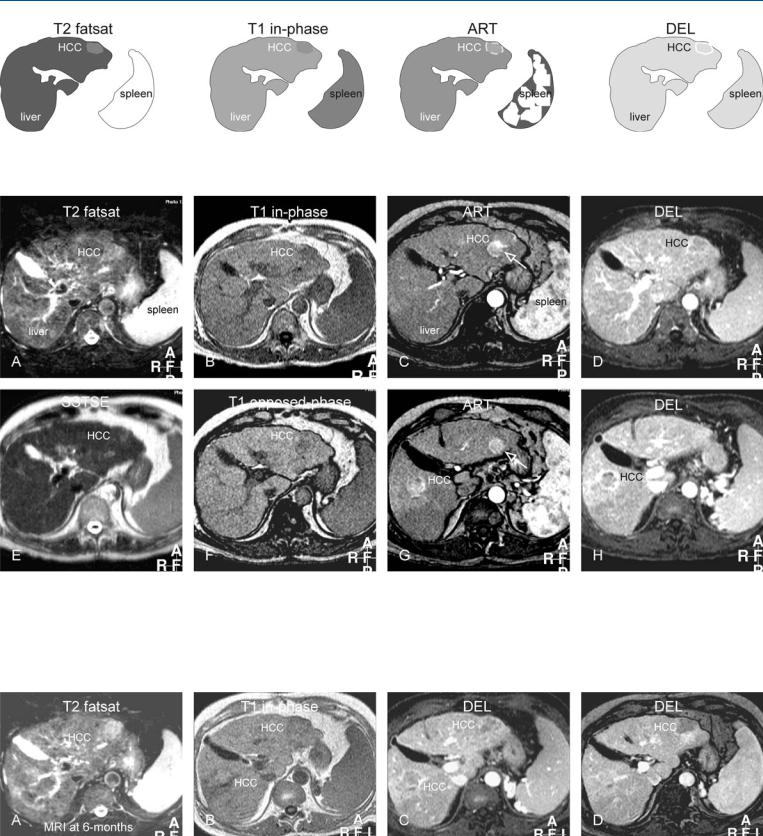
At MR imaging, the combination of hypointensity on T1-weighted images, hyperintensity on T2-weighted images, and diffuse heterogeneous enhancement is the most common appearance of HCC on MR images. Small HCCs ( 2 cm) are frequently isointense on both T1-weighted and T2-weighted images and may be detected on immediate gadolinium-enhanced images only (Figs. 50.1. 50.2). Fol- low-up may be considered in patients with suspicion of multiple HCC (Fig. 50.3).
Differential Diagnosis
In the setting of cirrhosis, high-grade dysplastic nodules, vascular shunts, and pseudolesions may have some overlap with small and developing HCC. Without any clinical evidence of liver disease and the lack of imaging signs of cirrhosis, focal nodular hyperplasia syndrome, hepatocellular adenomas, and multiple metastases should be considered.
50 HCC in Cirrhosis IX – Multiple Lesions Growing on Follow-up 107
Fig. 50.1. HCC, cirrhosis, multiple. T2 fatsat: HCC is only slightly brighter than the cirrhotic liver; T1 in-phase: HCC is only slightly darker than the cirrhot-
Fig. 50.2. HCC, cirrhosis, multiple lesions, MRI findings. A Axial TSE image (T2 fatsat): HCC is only slightly brighter than the cirrhotic liver and difficult to recognize, also because of ghost artifacts. B Axial in-phase image (T1 inphase): HCC is only slightly darker than the cirrhotic liver. C Axial arterial phase image (ART): HCC shows faint heterogeneous enhancement. Ghost artifact of the aorta (open arrow). D Axial delayed phase image (DEL): HCC
ic liver; ART: HCC shows faint heterogeneous enhancement; DEL: HCC shows washout with capsular enhancement
shows washout with capsular enhancement. E Axial SSTSE image (SSTSE): HCC is hardly visible within a cirrhotic liver with irregular contours. F Axial opposed-phase image (T1 opposed-phase): No fatty infiltration is present. G Axial arterial phase image (ART) at lower anatomic level shows a second HCC. Ghost artifact of the aorta (open arrow). H Axial delayed phase image (DEL): The second HCC also shows washout with capsular enhancement
Fig. 50.3. HCC, cirrhosis, multiple lesions, MRI findings at 6 months. A Axial TSE image (T2 fatsat): HCC has become brighter and larger in size. B Axial inphase image (T1 in-phase): HCC in the left liver is hypointense and HCC in the right liver is hyperintense to the liver. C Axial delayed phase image
(DEL): HCC in the right liver is larger with washout and capsular enhancement. D Axial delayed phase image (DEL): HCC in the left liver shows more washout