


72 Part IIB – Metastases: Non-Colorectal
34 Renal Cell Carcinoma Liver Metastasis
Renal cell carcinoma (RCC) is the 7th leading malignant condition among men and the 12th among women, accounting for 2.6 % of all cancers. The aim of preoperative imaging in RCC is to adequately assess tumor size, localization and organ confinement, to identify lymph node and/or visceral metastases, and to reliably predict the presence and extent of any thrombus of the vena cava. In 25 % of patients, advanced disease, including locally invasive or metastatic re- nal-cell carcinoma, is found at presentation. Moreover, a third of the patients who undergo resection of localized disease will have a recurrence. Median survival for patients with metastatic disease is about 13 months. Thus, there is a great need for more effective surgical and medical therapies. Nephrectomy may be warranted, even in the presence of metastatic disease. The detection of visceral metastases appears to be crucial since it has been shown that even patients with metastatic disease might benefit from radical nephrectomy followed by systemic immunotherapy. MR imaging provides more comprehensive locoregional evaluation of the primary lesion(s) including the distinction from concurrent (complicated) renal cysts, vascular invasion, and liver metastases.
Literature
1.Semelka RC, Shoenut JP, Magro CM, et al. (1993) Renal cancer staging: comparison of contrast-enhanced CT and gadolinium-enhanced fatsuppressed spin-echo and gradient-echo MR imaging. JMRI 3:597 – 602
2.Heidenreich A, Ravery V (2004) European Society of Oncological Urology: preoperative imaging in renal cell cancer. World J Urol 22:307 – 15
3.Mickisch GH, Garin A, van Poppel H, et al. (2001) Radical nephrectomy plus interferon-alfa-based immunotherapy compared with interferon alfa alone in metastatic renal-cell carcinoma: a randomized trial. Lancet 358:966 – 70
4.Figlin RA (1999) Renal cell carcinoma: management of advanced disease. J Urol 161:381 – 6
MR Imaging Findings
At MR imaging, renal cell carcinoma liver metastases appear low signal intensity on T1-weighted images and moderately high signal intensity on T2-weighted images with fat suppression. After administration of gadolinium, renal cell carcinoma liver metastases may show variable enhancement patterns including an intense homogeneous to heterogeneous enhancement in the arterial phase. In the portal and delayed phase the metastases often show washout and may become more heterogeneous (Figs. 34.1, 34.2).
Differential Diagnosis
Other hypervascular liver lesions including primary tumors as well as secondary tumors from other sources such as pancreas may have very similar appearance and need clinical correlation or US-guided biopsy for confirmation of proper diagnosis (Fig. 34.3).
Management
Surgical excision of a solitary metastasis in patients with advanced RCC is recommended in many cases, but this approach has not yet been proved to be effective in prolonging survival.
34 Renal Cell Carcinoma Liver Metastasis 73
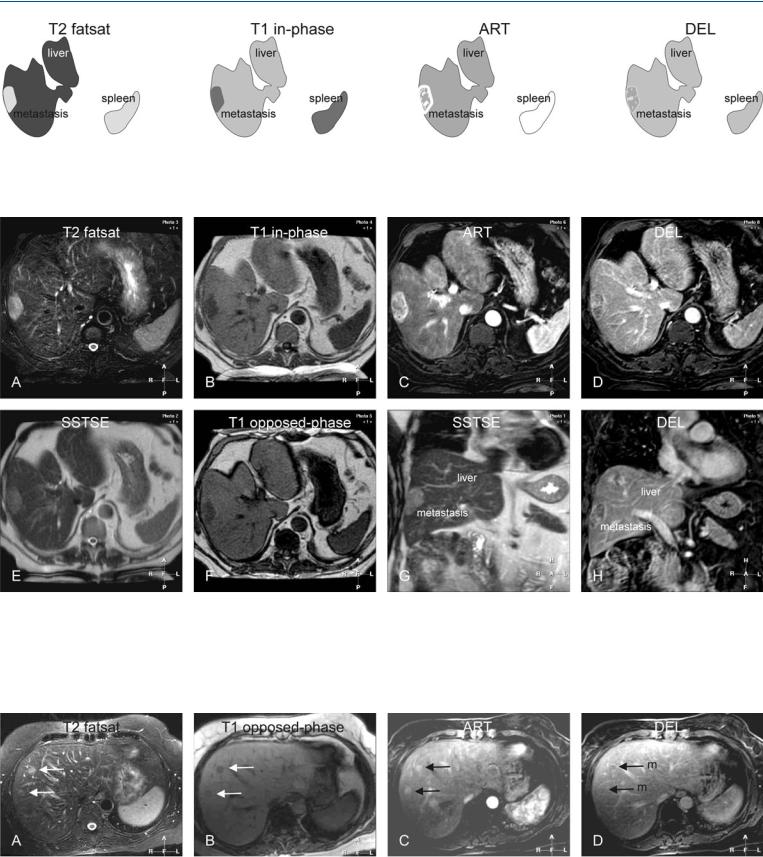
Fig. 34.1. Metastasis, renal cell carcinoma metastasis, drawings. T2 fatsat: Metastasis is hyperintense to the liver; T1 in-phase: metastasis is hypointense to the liver; ART: metastasis shows intense heterogeneous enhancement;
Fig. 34.2. Metastasis, renal cell carcinoma metastasis, MRI findings. A Axial TSE image (T2 fatsat): Metastasis is hyperintense to the liver. B Axial in-phase image (T1 in-phase): Metastasis is hypointense to the liver. C Axial arterial phase image (ART): Metastasis shows heterogeneous enhancement. D Axial delayed phase image (DEL): Metastasis shows some washout with persistent heterogeneous enhancement. E Axial SSTSE image (SSTSE): Metastasis is
DEL: metastasis shows some washout with persistent heterogeneous enhancement
slightly hyperintense. F Axial opposed-phase image (T1 opposed-phase) shows slight signal drop in the liver indicating subtle steatosis. Note that metastases are surrounded by persistent high perifocal signal due to compressed liver. G Coronal SSTSE image (SSTSE) shows the metastasis as a relatively bright lesion. H Coronal delayed image (DEL) shows the metastasis with persistent heterogeneous enhancement
Fig. 34.3. Metastases, pancreas carcinoma metastases (another patient), MRI findings. A Axial TSE image (T2 fatsat) shows two metastases that are slightly hyperintense to the liver (arrows). B Axial opposed-phase image (T1 op- posed-phase): metastases are hypointense to the liver (arrows). C Axial arte-
rial phase image (ART): metastases show faint, homogenous enhancement (arrows). D Axial delayed phase image (DEL) shows washout within lesions
(m).

Part II/IIC
Solid Liver Lesions |
II |
Primary Solid Liver Lesions in Cirrhotic Liver |
IIB |