


38 |
E. Hattingen and M. Warmuth-Metz |
|
|
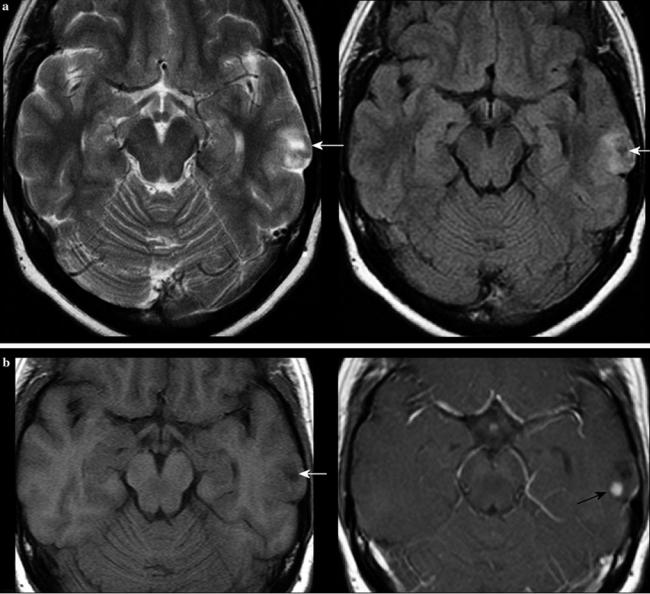
Fig. 33 The same patient as in Fig. 14c. Hypointense signals in T2WI might be due to hemorrhage, which is more often found in malignant brain tumors. The CCT yields strong calcifications which cause signal loss in T2*WI. The signal intensity of calcification may be hypointense
due to its diamagnetic properties, whereas the size and configuration of calcium salt deposits as well as its interactions with other paramagnetic cations may cause T1 shortening
gangliogliomas, the most frequent glioneuronal tumor, might show malignant transformation. Glioneuronal tumors are mostly located in the temporal lobe, especially in the temporomesial region, abutting the brain surface (Figs. 13 and 34). Cystic components and partial contrast enhancement is also found. The DNET may show little cysts which might have a typical hyperintense rim on FLAIR (Fig. 35). Tumors with cystic components (which might be indistinguishable from necroses) and nodular enhancing tumor abutting the brain surface in younger adults are suspicious for glioneuronal tumors. Other differential diagnoses include very rare tumors like pleomorphic xanthoastrocytoma, originating from subpial astrocytes, and astroblastomas (Fig. 36). These tumors are large, peripheral supratentorial tumors with
cystic and solid parts and a characteristic bubbly appearance (Fig. 29).
3Pediatric Brain Tumors
3.1Standard MRI
In children, the slice length should not exceed 4 mm. For small structures even much smaller slice lengths might be necessary. Although many surgical or radiotherapy treatment planning systems require three-dimensional sequences, these should only be additional to the core of standard imaging: It may be impossible to compare a tumor
MR Imaging of Brain Tumors |
39 |
|
|
Fig. 34 Young adult with incidental finding of a small tumor in the left temporal lobe abutting the brain surface with a cystic component (white arrows) adjacent to an enhancing nodule (black arrow). Histopathology revealed a ganglioglioma
on sequential SE scans with the same tumor on 3D scans or MPR series because the contrast behavior of tumors can differ considerably on these sequences (Pinker et al. 2007). An automatized 3D volume calculation of brain tumors can only be used in singleor limited-center studies because the acquisition parameters have to be uniform.
DWI with the additional calculation of the ADC allows not only the depiction of infarcted brain but also an estimation of cellular density in the absence of hemorrhage
(Kato et al. 2009). Together with the signal intensity on T2-weighted MRI, the ADC is a very useful tool for differential diagnosis (Kan et al. 2006). Susceptibility-weighted sequences are useful for the identification of calcification or blood degradation products. However, in pediatric brain tumors with the exception of craniopharyngiomas, this feature is of little importance compared to its value in the differentiation of adult high-grade gliomas (Zulfiqar et al. 2012; Tsuda et al. 1997; Pinker et al. 2007).
40 |
E. Hattingen and M. Warmuth-Metz |
|
|
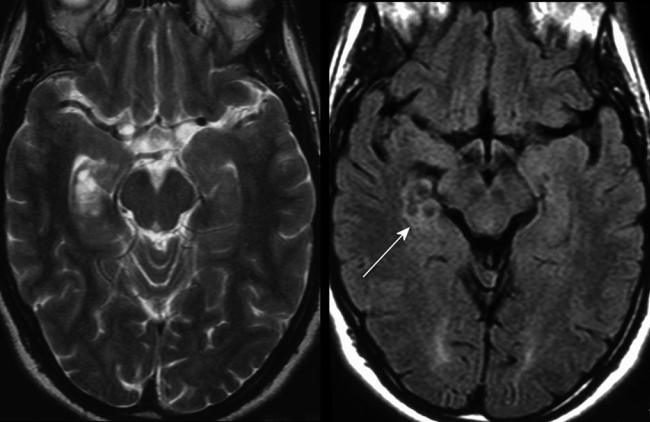
Fig. 35 The temporomesial DNET shows typical well-defined hyperintense rings on FLAIR sequence
3.2Differential Diagnosis of Common Pediatric Brain Tumors
Pilocytic astrocytomas are the most frequent brain tumors in children in all parts of the CNS. One of the main features on histopathology also relevant for imaging features is the low cellular density. They frequently take up contrast agent and might contain cystic components, which should not be mentioned as necroses. Necrotic components are clearly features of high-grade tumors like glioblastomas or of treatment-induced necrosis. The walls of tumor cysts may enhance (Fig. 37), and enhancement allows to differentiate pilocytic astrocytomas from hemangioblastomas, also termed as Lindau tumors. This entity is most frequently localized in the cerebellum, spinal cord, and rarely—espe- cially in adolescents and younger adults—in the supratentorial brain. It might consist of a pure nodule or a strongly enhancing nidus within a cyst. This similarity can create diagnostic problems in the discrimination from pilocytic astrocytomas (Beni-Adani et al. 2000). A hemangioblastoma can be safely excluded if cyst wall enhancement is
present (Bishop et al. 2008) (Fig. 38). If cyst wall enhancement is absent, there is no way to differentiate between hemangioblastoma and pilocytic astrocytoma with standard imaging. The reduced cellular density corresponds to a high T2 signal and high ADC values (Fig. 39) facilitating the differentiation from tumors with high cell density, e.g., medulloblastomas/ependymomas (Fig. 40), or—in the suprasellar or pineal region—to germ cell tumors always showing a cell density comparable to gray matter (Fig. 41). Unenhanced CT is also very helpful to assess cell density of pediatric brain tumors (Poretti et al. 2012) (Fig. 42). Among our own unpublished studies of far more than 100 patients with medulloblastomas undergoing CT without contrast enhancement, no tumor with hypodense CT values in the solid tumor parts was found. However, in supratentorial gliomas, an accurate differentiation between lowand high-grade gliomas is not possible because the cell density of the solid components in high-grade gliomas usually remains below the cell density of PNETs or ependymomas (Fig. 43). Other ominous features like inhomogeneous texture or an increase of perifocal edema (Fig. 44) have to be taken into
MR Imaging of Brain Tumors |
41 |
|
|
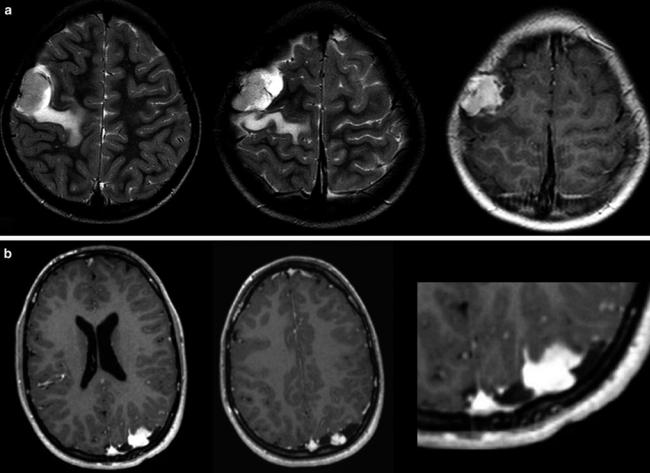
Fig. 36 Tumors abutting the brain surface in young adults, modeling the adjacent bone. Both tumors have pronounced larger enhancing tumor nodules together with small cystic areas. Histopathological
diagnoses yielded an astroblastoma WHO grade II (a) and a xanthogranulomatous astrocytoma grade II (b)
account. The diagnosis of gliomatosis cerebri, which may vary on histology from WHO grade II to IV, is based on the involvement of more than two lobes of the brain (Fig. 45).
To diagnose a diffuse intrinsic pontine glioma (DIPG), typical clinical complaints in addition to typical infiltrative appearance on MRI are required (Fig. 46). Key features are an extension of more than 50 % of the pontine cross-sectional area and a clear tumor origin and center in the pons (Fischbein et al. 1996) and not other parts of the brainstem, e.g., medulla oblongata, where low-grade gliomas predominate. Contrast enhancement at the time of diagnosis might have a prognostic importance (Poussaint et al. 2011). Cysts are extremely rare and can be a sign for a low-grade histology (Fig. 47), indicating the need of a histological clarification. If biopsy does not seem to be feasible, a close follow-up is mandatory. In neurofibromatosis type 1 as well, focal and also seemingly typical DIPG can exist but usually show a much more benign clinical course (Fig. 48).
In the suprasellar compartment, the differentiation between the frequent tumors in children in this localization
like craniopharyngioma, LGG, and germ cell tumor is usually possible on the basis of conventional MR/CT imaging (Table 3). Small germ cell tumors might be indistinguishable from a hypothalamo-pituitary lesion in Langerhans cell histiocytosis (Makras et al. 2006). Adamantinous craniopharyngiomas are the typical craniopharyngiomas in children and show frequently calcification and cysts. CT without contrast is the additional method of choice (Tsuda et al. 1997; Warmuth-Metz et al. 2004a, b) (Fig. 49) and can be centered on the tumor without touching the radiosensitive eye lens. Extreme dose reduction in order to protect the child should be avoided because very small calcifications might be detectable only on the soft tissue reconstruction, which needs a higher dose of radiation for adequate image quality. Varying with the individual position of the craniopharyngioma, a loss of the physiological bright posterior pituitary lobe (PPL) signal on the unenhanced T1-weighted MRI is possible and therefore sagittal thin-slice T1-weighted images are very useful (Fig. 50). A loss of the bright PPL signal indicates the disturbance of the hypothalamic-PPL axis.
42 |
E. Hattingen and M. Warmuth-Metz |
|
|
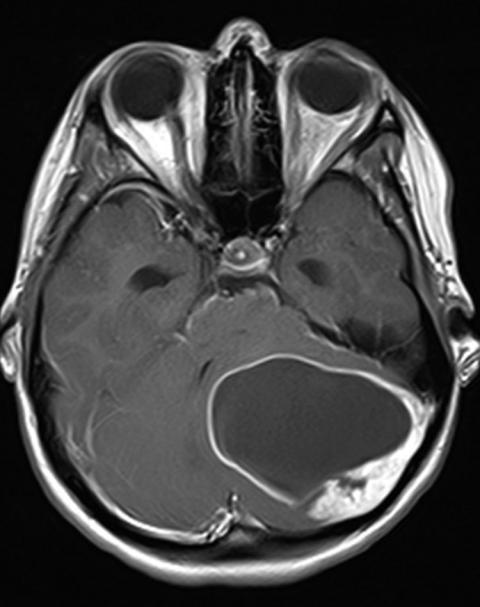
Fig. 37 Enhancement of the cyst wall as shown in this cerebellar pilocytic astrocytoma can be useful for the differential diagnosis between glioma and hemangioblastoma. Many pilocytic astrocytomas do not show cyst wall enhancement. If so, pilocytic astrocytomas should be assumed because hemangioblastomas almost always lack cyst wall enhancement
Germ cell tumors in a suprasellar position almost always have no T1-hyperintense signal in the PPL (Di Iorgi et al. 2012). Due to a high ratio between cell nuclei and cytoplasm, these tumors usually show a T2-signal comparable to gray matter, a restricted diffusion and a regular, frequently intense contrast enhancement (Liang et al. 2002; Sumida et al. 1995). The various types of germ cell tumors with the exception of the typically inhomogeneous teratomas cannot be differentiated from each other on MRI.
Pilocytic astrocytomas of the chiasm/hypothalamus are tumors with a low cellular density and therefore show a high T2 signal (Poretti et al. 2012), no restricted diffusion,
and hardly ever a loss of the physiologic bright PPL signal. In very young children, tumors in this localization may be accompanied by a meningeal dissemination with an increase of protein but without tumor cell detection in the CSF (Gnekow et al. 2012).
Spinal tumors cannot be differentiated on the basis of MRI features with rare exceptions. In general, all tumors of the CNS can be localized within the spinal cord. Statistically in children, especially the younger ones, astrocytic tumors predominate (Jallo et al. 2003). Ependymomas are very vascular. Only rarely a leptomeningeal siderosis or the unusual presence of hemosiderin capping (cap sign)