

34 |
E. Hattingen and M. Warmuth-Metz |
|
|
Fig. 29 Two similar tumors with enhancing nodules abutting the brain surface and large cysts: The tumor of the older patient shows some edema, whereas the tumor of the young patient lacks any edema. The
older patient only had one seizure, whereas the young patient had epilepsy with complex partial seizures. The older patient had a GBM; the young patient had a pleomorphic xanthoastrocytoma
show more or less pronounced calcification on CCT. Further, it should be performed in patients with MRI contraindications. CCT may also be helpful to characterize cell density of a brain tumor in children (Sect. 3). In adults PCNSL are typical tumors with cortex-isodense appearance in contrast to most of the gliomas which are hypodense on CCT.
2.6Case Illustrations
Although MRI has limited diagnostic accuracy, there are some clues to narrow differential diagnosis. These criteria should always include or rather begin with patient’s age considering that the likelihood of malignancy in adulthood increases with age (Fig. 29).

MR Imaging of Brain Tumors |
35 |
|
|
Fig. 30 Two similar histopathologically proven astrocytomas in the right parietal lobe infiltrating the cortex, both without contrast enhancement: The gyri are bloated and gray-white matter junction is effaced.
The tumor in (a) was a astrocytoma WHO grade III, whereas in (b) an astrocytoma WHO grade II was found
36 |
E. Hattingen and M. Warmuth-Metz |
|
|
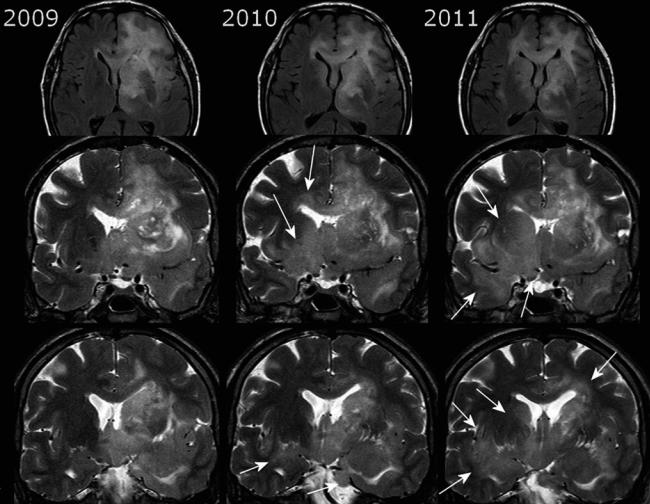
Fig. 31 The gliomatosis of the left hemisphere infiltrating the corpus callosum was treated with radiation in 2009. In 2010, the mass effect of the left-sided tumor declined, but tumor progressed by infiltrating the right temporal white matter, the insula, the basal ganglia, and
hypothalamus bilaterally (white arrows). Coronal T2WI depicts the infiltration ways en face minimizing partial volume effects of axial slices, and further they visualize the blurring of gray-white matter junction due to the tumor infiltration
1.WHO grade II and III gliomas
Most low-grade gliomas or gliomas with secondary
malignant transformation infiltrate cortical structures (Fig. 30). A preferential localization of low-grade astrocytoma is the frontotemporal lobe with involvement of the temporal stem, the temporomesial structures, and the insula. The infiltration way often follows white matter tracts like the anterior commissure and the corpus callosum. Coronaloriented T2WI are very helpful in depicting the extent of low-grade tumorsand to detect tumor progression in the follow-up (Fig. 31). Due to the diffuse infiltration pattern, low-grade tumors do not expand spherically, but infiltrate the anatomical structures often without severally
distorting them. Therefore, size measurement of these brain tumors is of limited value.
WHO grade III oligodendrogliomas are i.a. defined by microvascular proliferation and necrosis which give them the appearance of a highly malignant GBM (Fig. 32). WHO grade II oligodendrogliomas may already appear malignant due to their inhomogeneous tumor areas with cysts, calcifications, and hemorrhage (Fig. 33).
2.Glioneuronal tumors
The hallmarks of these tumors are the younger patient age
(children and young adults) and the high association with epilepsy with complex partial seizures. Although mostly benign, one should be aware that the glial component of

MR Imaging of Brain Tumors |
37 |
|
|
Fig. 32 Very inhomogeneous tumor with cystic areas, irregular, and patchy enhancement of the margins. It has the appearance of GBM, except for the small surrounding edema which is not typical for large
necrotic GBMs (a, b). The CCT (a) shows calcification which yields faint hyperand hypointense signal changes in precontrast T1WI (c); see also Fig. 33. Histopathology yielded an oligodendroglioma WHO grade III