

MR Imaging of Brain Tumors |
33 |
|
|
Fig. 28 The astrocytoma WHO grade II 2 years after surgery with residual peri-insular tumor on FLAIR (a) and T2WI (b): Some tumor areas (arrows) might be missed on FLAIR due to the T1-effect yielding intermediate signal in contrast to the hyperintense signal on T2WI
The most attention apart from contrast enhancement is given to Fluid-attenuated inversion recovery
(FLAIR) sequences. Isovolumetric 3D FLAIR sequences allow for multiplanar reconstructions and obviate partial volume effects or artifacts of sequential 2D FLAIR. However, some basic physics of this sequence should be considered: FLAIR signal is not only influenced by the T2 relaxation time (T2-weighted) but also by the Tl relaxation time (Tl-weighted). Further, the contrast between gray and white matter and thus the delineation of anatomical structures may be inferior to T2WI. Therefore, signal changes may be more ambiguous on FLAIR than on T1WI and T2WI, and subtle infiltration of gray matter (cortical ribbon sign) may be less obvious compared to T2WI (Fig. 28), yielding
differentiation between tumor and vasogenic edema more difficult. Therefore, FLAIR should not replace but supplement T2WI.
Susceptibility-weighted imaging (SWI) detects small veins and extravascular blood products including tumorassociated microhemorrhages. Recently, it has been shown that SWI after i.v. application of contrast agent visualizes architecture of tumor vessels. Increasing numbers of small vessels and intratumoral susceptibility signals seem to be hallmarks of high-grade gliomas (Pinker et al. 2007) and help to distinguish them from lymphomas.
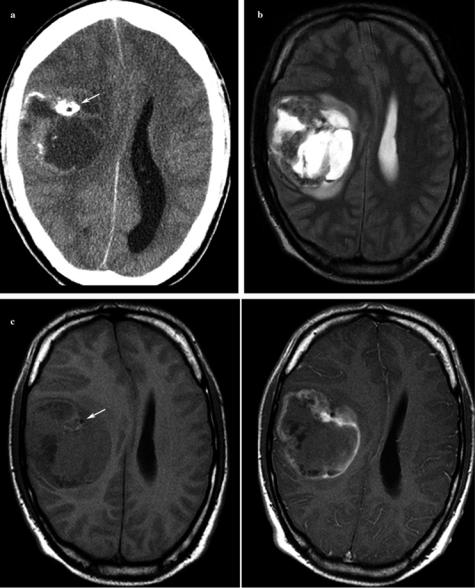
Computer Tomography
CCT may be indicated to detect calcification which narrows the differential diagnosis. 70–90 % of oligodendrogliomas