

Laparoscopic Adjustable Band |
239 |
Anastomotic Ulcers. Anastomotic ulcers are usually secondary to a pouch larger than 30 cm3 with increased acid secretion, a gastro-gastric fistula are found in a patient who continues to smoke postoperatively. In most cases, ulcers can be treated with proton pump inhibitors and cessation of smoking; however, if the ulcer results in perforation, the patient needs to be taken to the operating room. A Graham’s patch with or without closure of the hole is the treatment of choice. If the symptoms persist, another option is to redo the anastomosis after the inflammation has subsided.
Stricture. Constant vomiting and intolerance to food, more commonly than dumping syndrome, is due to stricture at the gastrojejunostomy. It usually manifests itself at the end of the second postoperative month. A postoperative stricture is normally diagnosed with endoscopy revealing an anastomosis less than 8 mm in diameter; this can often be treated with a single dilatation to a diameter of 1.5 cm, although a second dilatation is occasionally needed. In our experience, once we added an additional 7–8 mm to the diameter of the anastomosis by starting the gastojenostomy 1 cm above the inferolateral corner of the pouch, no strictures have been seen (Fig. 14.23).
OR Set Up
The patient can be placed in either the supine or lithotomy position. The benefit of the supine position is a faster set up and decreased risk of pressure on the thighs from the buttock holders. If the patient is placed in lithotomy position, the OR set up is exactly as for the Nissen procedure with one monitor above the patient’s head and one on the left side of the patient.
Technique
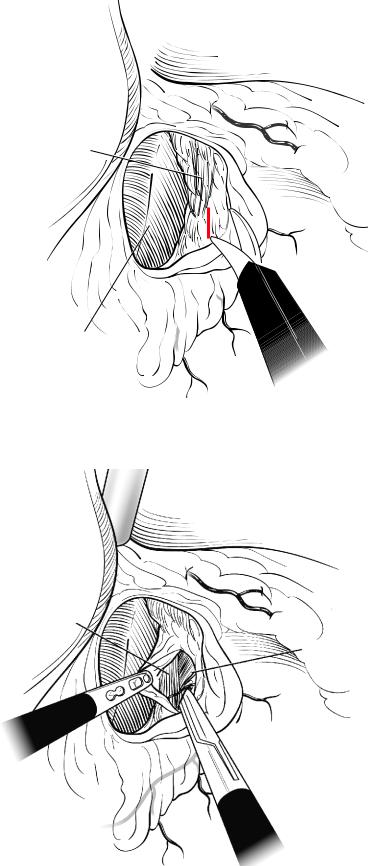
We use a five-trocar technique for the lap band (Fig.14.37).The trocar placement is the same as in the fundoplication. The first step is retraction of the left lobe of the liver. In the case of a very large accessory left hepatic artery barring the pars flaccida, it is possible to dissect the artery on either side to avoid ligating it. In the case of an artery that blocks access to the hiatus, it is possible to clamp the artery and monitor the effect on the liver. If there is no ischemia, the artery can be divided. The avascular aspect of the pars flacida is opened lateral to the nerve of Latarjet (Fig. 14.38). The membrane lying over the medial edge right crus is opened very low, near the crural decussation (Fig. 14.39), and by gently using a grasper from left to right, a small window is created under the esophagus and below the left crus (Fig. 14.40). We do not like to insert instruments blindly behind the esophagus, as is commonly performed rather, we prefer to see this window created under direct vision to avoid injury to the esophagus. The angle of His is opened using the harmonic shears. A special dissector is placed in this window (Fig.14.41).At this point,a fifteen millimeter trocar allows the insertion of the Realize Band (Ethicon Endo-Surgery Inc, Cincinatti, OH) (Fig. 14.42). The knotted thread is placed in the special dissector, and this permits the band to be pulled behind the esophagus and closed just under the decussation (14.43).All these cases are done using the pars flaccida technique to minimize slippage.Once the band is closed making sure that the buckle is facing toward the liver and the angulation is ideal at 45 degrees towards the left (Fig. 14.44), the stomach is used to imbricate the band to further minimize the slippage.
Laparoscopic
Adjustable
Band

240 |
Chapter 14 Bariatric Surgery |
S
CA
|
10E |
|
5 |
|
5 |
|
15 |
||
|
D |
|||
A |
10 |
B |
||
FA |
||||
|
||||
|
C |
|
||
|
|
|
Fig. 14.37 Trocar position for lap band surgery. C camera; A left hand of surgeon; B right hand of surgeon and site of introduction of the port (15 mm); D assistant’s grasper; E liver retractor. S surgeon; CA camera assistant; FA first assistant
Left margin of stomach
under fat layer
Caudate lobe of liver under pars accida
Fig. 14.38 Opening the avascular aspet of the pars flaccida (“Pars Flaccida” technique)
Laparoscopic Adjustable Band |
241 |
Rt. crus under lateral fat of stomach
Caudate lobe
Fig. 14.39 Incision of the peritoneal layer over the right crus of the diaphragm
Rt. crus
L. crus
Fig. 14.40 Dissection and creation of the retroesophageal tunnel under the left crus, near the
decussation of the crura

242 |
Chapter 14 Bariatric Surgery |
Fig. 14.41 The Goldfinger dissector is passed through the retroesophageal tunnel
Fig. 14.42 Passage of the band in the retroesophageal tunnel

Laparoscopic Adjustable Band |
243 |
Fig. 14.43 Band placed according to the “Pars Flaccida” technique
Fig. 14.44 The band is closed and the buckle is placed towards the caudate lobe of the liver, thus leaving the inflated chamber on the gastric wall