


Appendectomy 7
OR Setup and Port Placement |
Acute |
The patient is placed in the supine position with the left arm or both arms tucked.A foley |
Appendicitis |
catheter is always placed as in other pelvic or lower abdominal procedures to decrease |
|
the risk of injury to the bladder during port placement. The surgeon and the assistant |
|
both stand on the left side of the patient facing the monitor located on the right side of |
|
the patient (Fig. 7.1). |
|
Pneumoperitoneum is created in the standard fashion using either the Hasson |
|
technique or a Veress needle. Care must be taken in patients who have had a longer |
|
course of disease if using a Veress needle, as the inflammation of the omentum and sur- |
|
rounding small bowel increase the risk of injury to the small bowel or other structures. |
|
The ports are inserted in an extended triangulation fashion. The laparoscope is |
|
placed at the umbilicus. Two 5 or 10 mm ports are inserted, one in the left lower quadrant |
|
in a position corresponding but opposite to McBurney’s point, and the second is placed |
|
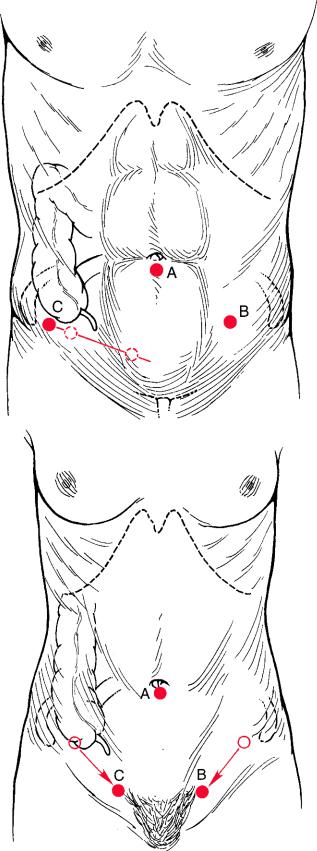
in a suprapubic position. In a male patient, the right trocar is inserted in a position cor- |
|
responding to the left (Fig. 7.2a). In a female patient, both trocars can be hidden in the |
|
pubic hair line if cosmesis is an issue (Fig. 7.2b). If an additional trocar is needed for |
|
bowel retraction or suctioning, a 5-mm port can be placed in the right upper quadrant. |
|
Then the patient is placed in Trendelenburg position with the right side up. |
|
Care must be taken to avoid a “knitting needle” effect between instruments and the |
|
laparoscope; all ports should be placed in such a way that they have free movement and |
|
do not interfere with one another. The body habitus of the patient will influence place- |
|
ment of the ports to achieve this goal. |
|
N. Katkhouda, Advanced Laparoscopic Surgery,
DOI: 10.1007/978-3-540-74843-4_7, © Springer-Verlag Berlin Heidelberg 2011

120 |
Chapter 7 Appendectomy |
Fig. 7.1 Patient position for appendectomy. S surgeon; CA camera assistant
The surgeon’s left hand operates the Babcock grasper to retract the cecum or the tip of the appendix (if the appendix is in its usual paracecal position). The surgeon’s right hand operates a Kelly grasper to create windows in the mesoappendix. If the appendix is not clearly identifiable because it is retrocecal, the cecum needs to be mobilized and retracted medially (Fig. 7.3).
Acute Appendicitis |
121 |
a
b
Fig. 7.2 Port positions for (a) a male patient and (b) a female patient. A telescope; B surgeon’s
right hand; C surgeon’s left hand