

110 |
Chapter 6 Gastric Surgery |
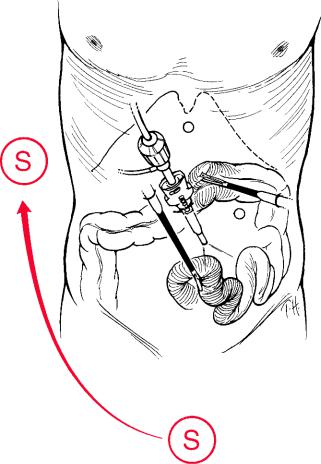
Perforated
Duodenal Ulcer
Fig. 6.10 Exposure of the jejunum in gastrectomy. The surgeon (S) moves to the right side of
the patient and the scope is oriented down towards the pelvis
If the patient’s condition is stable, and peritonitis is diagnosed within 12 h of onset, it is possible to perform an operation laparoscopically (after 12 h, chemical peritonitis will give way to bacterial peritonitis presenting with severe sepsis, and laparoscopy may not be recommended in this situation). Care should be taken not to use a high insufflation pressure which could push intra-abdominal bacteria into the blood stream leading to bacteremia and septic shock. Pneumoperitoneum pressure should be maintained below 11 mmHg.
Locating the Perforation
Pneumoperitoneum is created in the traditional way. Four ports are then inserted using the triangulation concept, to form a diamond-shape. The surgeon stands between the legs of the patient, with the first assistant to the right and a second assistant to the left. The lead surgeon thus works comfortably with two hands, triangulated between the cameras (Fig. 6.12).

Perforated Duodenal Ulcer |
111 |
Fig. 6.11 Exteriorization of the stomach and jejunum for side-to-side stapled Biliroth II gastrojejunostomy
Fig. 6.12 Port positions for perforated duodenal ulcer. A umbilicus; B surgeon’s right hand; C surgeon’s left hand, D irrigation and suction and/or fan retractor for liver retraction. S surgeon; FA first assistant; CA camera assistant

112 Chapter 6 Gastric Surgery
The gallbladder, which usually adheres to the perforation, is retracted by the surgeon’s left hand and moved upwards. The gallbladder is passed to the assistant using the subxyphoid port, which is placed to the right of the falciform ligament. The exposed area is checked and the perforation is usually clearly identified as a pinpoint hole on the anterior aspect of the duodenum, which has been covered by the fundus of the gallbladder. If the perforation is larger than the tip of the irrigation suction device (7–8 mm) and the crater is inflamed and friable, it is recommended to convert to an open procedure to safely close the perforation following a Kocher maneuver.
Abdominal Washout
The next step is careful and thorough irrigation and suction of all the intra-abdominal fluid. This should be done before the closure of the perforation to avoid any inadvertent disruption of the sutures during the washout. This is a tedious but essential task and needs patience. To irrigate and aspirate the whole abdomen requires about 10 L of saline mixed with local antibiotics.
Each quadrant is cleaned methodically, starting at the right upper quadrant, going to the left, moving down to the left lower quadrant, and then finally over to the right. Special attention should be given to the vesicorectal pouch. Fibrous membranes are removed as much as possible, since they may contain bacteria. The use of a 2 × 2 gauze introduced through one of the ports is helpful. However, if taking out fibrin attachments means injuring the intra-abdominal viscus, it should be done conservatively. This is a judgment call.
Management of the upper quadrants requires the surgeon to stand between the patient’s legs. For the lower quadrants the surgeon should move to the right side of the patient, who should be tilted in Trendelenburg to give access to the pelvis. Special careshould be taken to irrigate and aspirate between the loops of the small bowel. Once all this has been done, the patient is tilted back to the normal position for the surgeon to close the perforation.
Closure of the Perforation with an Omental Patch
The perforation is closed using an omental patch (Fig. 6.13).
An intracorporeal technique is preferred to avoid undue tension on the closure. It is advisable to insert the omental patch in the knot (true Graham patch), rather than use the tails of the knot to fix the patch as a result of which a small space remains between the knot itself and the omental patch, thereby diminishing the efficacy of the patch (Fig. 6.14a, b). The classic technique follows the same rules as with the original open Graham patch. The assistant holds the omental patch while the surgeon uses both hands to knot the ties. It is not necessary to place an abdominal drain if the procedure has been conducted appropriately.

Perforated Duodenal Ulcer |
113 |
Fig. 6.13 Closure of the perforation
Postoperative Course
The patient ambulates the next day and liquids are started in moderation on the third day; if the vitals are normal and there is no sepsis, the patient is discharged on an antihelicobacter regimen for 14 days starting that day. We do not routinely order a gastrographin swallow.
114 |
Chapter 6 Gastric Surgery |
a
b
Fig. 6.14 Omental patches: (a) a patch plugging the hole between the threads of the stitch, and (b) a less efficacious arrangement with the patch between the tails of the tied knots