

186 |
Chapter 12 Splenectomy (Total and Partial) and Splenopancreatectomy |
Port Placement
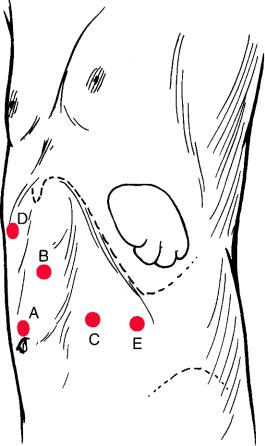
Four to five 12 mm ports are needed for this operation (Fig. 12.5). Following insufflation using a Veress needle, the first trocar is inserted in the left upper quadrant approximately five fingerbreadths below the costal margin, moving the camera closer to the spleen. This will permit full exploration of the abdominal cavity to check for the presence of accessory spleens and other intra-abdominal lesions that might require laparoscopic management.
One port is inserted on each side of the umbilical port in a triangulated manner, for the right and left hands of the surgeon. Another trocar is inserted laterally under the left costal margin for the first assistant. An optional subxiphoid trocar can be inserted for an irrigation/suction device or for a fan retractor used by the camera assistant if needed.
Fig. 12.5 Port positions for laparoscopic splenectomy: A umbilical telescope; B surgeon’s left
hand; C surgeon’s right hand; D subxiphoid port for irrigation/suction or an assistant’s grasper;
E first assistant’s grasper
Classic Laparoscopic Splenectomy |
187 |
Surgical Anatomy
Vascularization of the spleen may be of the distributed type (Fig. 12.6a) or the nonbranching variant (Fig. 12.6b). Knowledge of the patient’s vascular anatomy will help decide on the most appropriate dissection technique. The terminal branches of the splenic artery are depicted in Fig. 12.7. Knowledge of the anatomy of the spleen is critical, and two special features are of interest. First, as a rule, notched spleens and those with prominences have more entering arteries than those with smooth borders (usually distributed type). Second, the tail of the pancreas lies close to the hilum of the spleen and is in direct contact with the spleen in about 30% of cases, and within 1 cm of the spleen in 40%. Caution is therefore recommended before firing a linear cutter across the hilar vessels.
a
b
Fig. 12.6 Vascularization of the spleen: (a) distributed type with multiple splenic notches, and (b) magistral type with few splenic notches