


Splenectomy 12
(Total and Partial) and
Splenopancreatectomy
Preoperative Requirements and Workup
Laparoscopic splenectomy is a difficult procedure that should only be performed by an experienced laparoscopic surgeon or under the direct supervision of such a surgeon. As always, the entire team should be adequately prepared.
The surgeon should check the instrument set personally to ensure that everything is available, specifically clip appliers, atraumatic graspers, liver fan retractors, and an irrigation suction machine with the capacity for hydrodissection. An open tray with a number 10 or 20 blade should be immediately available in case there is a need for conversion. Harmonic shears (Ethicon Endosurgery Inc.) are especially useful because they can reduce the number of clips used during division of the short gastric vessels, and can also function as a grasper.
It is essential that patients presenting with idiopathic thrombocytopenic purpura (ITP) are worked up appropriately by the referring hematologists. The anesthesiologist must make sure that there is a suitable blood and platelet supply in the operating room prior to the start of the procedure.An orogastric tube is placed to decompress the stomach.
The patient should be vaccinated against pneumococcus, H. influenza and menningococcus (triple vaccine) at least 2 weeks prior to surgery.
Classic
Laparoscopic
Splenectomy
N. Katkhouda, Advanced Laparoscopic Surgery,
DOI: 10.1007/978-3-540-74843-4_12, © Springer-Verlag Berlin Heidelberg 2011
182 |
Chapter 12 Splenectomy (Total and Partial) and Splenopancreatectomy |
Patient Positioning
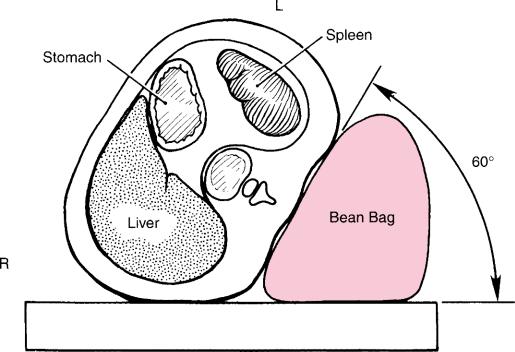
Proper patient positioning is a critical step. The patient is safely secured on a bean-bag with the left side up at a 60° angle in reverse Trendelenberg and the left arm positioned as for a left lateral thoracotomy (Fig. 12.1). This allows gravity to retract the abdominal organs and maximize the working space.This is the“hanging spleen”technique described by Delaitre and Gagner. The surgeon stands on the patient’s right side facing the left monitor, with the camera assistant on the same side sitting on a stool to his left to avoid a conflict with the elbows of the surgeon. The first assistant is on the opposite side, but the three members of the team all look at the left monitor to avoid mirror imaging and discoordination of the critical first assistant (Fig. 12.2).
When the trocars are inserted, the patient is positioned in reverse Trendelenburg. Combined with a 60° tilt, this position has two important effects. First, gravity pulls the stomach and small bowel in a rostral direction out of the operative field.Second,the spleen is kept hanging from the diaphragm by its phrenic attachments, thus placing the gastrosplenic vessels under tension, simplifying dissection and division of the vessels later in the operation (Fig. 12.3). In the anterior approach, the hilar vessels are controlled first, and the phrenic attachments are divided at the end of the operation. In contrast, with a posterior approach, the lateral attachments are divided first, the spleen is mobilized laterally and the hilar vessels are controlled later, as done in open surgery (Fig. 12.4).
Fig. 12.1 The patient’s position for laparoscopic splenectomy

Classic Laparoscopic Splenectomy |
183 |
Fig. 12.2 Operating room set up for laparoscopic splenectomy. S surgeon; FA first assistant; CA camera assistant sitting on a chair

184 |
Chapter 12 Splenectomy (Total and Partial) and Splenopancreatectomy |
a
b
c
Fig. 12.3 Effects of reverse Trendelenburg and 60° elevation: (a) splenic pedicle put under tension; (b) stomach falls down; (c) splenic flexure put under strain

Classic Laparoscopic Splenectomy |
185 |
a
b
Fig. 12.4 (a) Open splenectomy, and (b) laparoscopy (The “hanging spleen” technique). Numbers depict stages of the operation