

CASE
22Intracranial arteriovenous malformation
Jinendra Ekanayake
 Expert commentary Neil Kitchen
Expert commentary Neil Kitchen
Case history
A 54-year-old right-handed man was admitted with a 2-week history of left-sided headaches, visual disturbance, and difficulties with short-term memory. Examination revealed a right-sided temporal hemianopia.
Nine years previously, following a brief loss of consciousness at home, investigations had revealed a left-sided occipital arteriovenous malformation (AVM) with a 3.5-cm nidus, and associated deep venous drainage (Spetzler–Martin Grade 4). He remained entirely asymptomatic following this event, which was diagnosed as an unrelated vasovagal episode. It was initially decided that the management should be conservative, given the incidental discovery of the AVM.
 Learning point Surgical operability and the Spetzler–Martin grade
Learning point Surgical operability and the Spetzler–Martin grade
The Spetzler–Martin classification (1986) was proposed as a means of defining surgical operability [1]. It is based on three components—nidus size, venous drainage, and proximity to eloquent brain regions. Eloquent brain is given a somewhat broad description, including primary motor, sensory, visual and language cortices, as well as the thalamus, hypothalamus, brainstem, and cerebellar peduncles.
Table 22.1: The percentage of patients with a major neurological deficit (defined as hemiparesis aphasia, and/or hemianopia) increases as the Spetzler–Martin grade rises.
Table 22.1 Correlation of AVM grade with surgical results*
Grade |
No. cases |
No deficit |
|
Minor deficit |
|
Major deficit |
Death (%) |
||||
|
|
No. |
% |
|
No. |
% |
|
No. |
% |
|
|
|
|
|
|
|
|
||||||
|
|
|
|
|
|
||||||
|
|
|
|
|
|
|
|
|
|
|
|
I |
23 |
23 |
100 |
0 |
0 |
0 |
0 |
0 |
|||
II |
21 |
20 |
95 |
1 |
5 |
0 |
0 |
0 |
|||
III |
25 |
21 |
84 |
3 |
12 |
1 |
4 |
0 |
|||
IV |
15 |
11 |
73 |
3 |
20 |
1 |
7 |
0 |
|||
V |
16 |
11 |
69 |
3 |
19 |
2 |
12 |
0 |
|||
Total |
100 |
86 |
86 |
10 |
10 |
4 |
4 |
0 |
|||
|
|
|
|
|
|
|
|
|
|
|
|
*Exceptions to this include if the patient has repeated haemorrhages, or progressive neurological deficit, the presence of flow-related aneurysms (amenable to surgery or endovascular treatment) and steal-related deficits (amenable to endovascular treatment) [2].
The grade is the sum of the three individual components scoring AVMs from I to V (Table 22.2). A further grade has been proposed, VI, to define ‘inoperable’. Despite criticisms related to nidus
heterogeneity, eloquence, and infratentorial AVMs, the system has been prospectively validated and
remains in common usage.
(continued)
216 |
Challenging concepts in neurosurgery |
|
|
|
|
Table 22.2 Spetzler–Martin grading scale for AVMs |
|
|
|
|
|
|
|
Feature |
Score |
|
|
|
|
|
|
<3 cm |
1 |
|
|
3–6 cm |
2 |
|
|
>6 cm |
3 |
|
|
|
|
|
|
Location |
|
|
|
|
|
|
|
Non-eloquent cortex |
0 |
|
|
In/ adjacent to eloquent cortex |
1 |
|
|
|
|
|
|
Venous drainage |
|
|
|
|
|
|
|
Superficial only |
0 |
|
|
Deep |
1 |
|
|
|
|
Spetzler and Ponce have proposed a recent revision (2011) to this classification to reflect treatment strategies (Table 22.3) [2]. The grouping of the grades into a three-tier system was based on a pooled analysis of outcome in 1476 patients taken from seven surgical series. Predictive accuracies for surgical outcomes were found to similar when comparing surgical outcomes between the five-tier and threetier system [2,3].
Table 22.3 SpetzlerMartin grading scale for AVMs
Class |
Spetzler-Martin Grade |
Treatment |
|
|
|
A |
I &II |
Microsurgery |
B |
III |
Multimodality |
C |
IV & V |
No treatment* |
|
|
|
 Expert comment Unruptured AVMs—to treat or not to treat?
Expert comment Unruptured AVMs—to treat or not to treat?
Current best evidence in relation to treatment is from the ARUBA trial (A Randomised Trial in Unruptured Brain Aneurysms) reported by Mohr et al (2013) [4]. It was a prospective, parallel-design randomized controlled trial (NHS class A) which was stopped early, with a follow-up of 33 months. Eligibility was age 18 years or over, no previous haemorrhage or intervention, in patients with brain AVMs (bAVMs) considered suitable for obliteration. 226 patients were recruited between 2007–2013; 114 patients were randomised to intervention, 109 patients to best medical management (7 patients crossed to the intervention arm, without suffering a bleed). 5 were treated with surgery, 30 with embolisation, 31 with radiotherapy, 28 with a multimodality approach. The primary outcome measured were symptomatic stroke or death; secondary outcome measures were clinical impairment, defined
as 2 or higher on the modified Rankin Scale.35/114(30.7%) patients in the treatment arm vs 11/109 (10.1%) patients in the medical arm reached the primary endpoint. 17/109 (38.6%) treated patients, and 6/109 (14%) of the patients managed medically reached the secondary endpoint. The authors concluded that medical management was therefore superior to intervention for unruptured bAVM patients at 33 months.
Russin and Spetzler (2014) provided a critique of the study and its findings, citing design flaws, lack of standardisation of the treatment arm , and inadequate study detail (i.e. 726 patients were eligible, 226 patients were enrolled177 patients were managed outside of the randomisation process) [5].
Nonetheless, the findings of the ARUBA trial provide important evidence on the management of unruptured aneuryms, and is supported by the Scottish Intracranial Vascular Malformation Study (SIVMS) which was carried out between 1999–2003. This was a smaller prospective observational study, with a 3 year outcome, which found an increased risk of a poor outcome in patients receiving treatment, and those with large AVMs [6].
Case 22 Intracranial arteriovenous malformation |
217 |
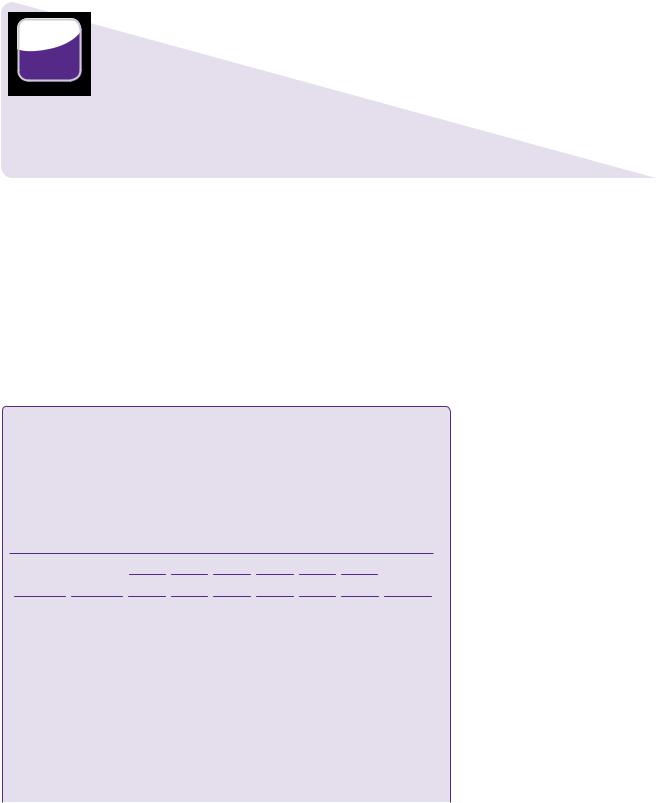
On his most recent admission, CT imaging once again confirmed the presence of the AVM. There was no evidence of an intracranial bleed or brain swelling associated with the AVM.
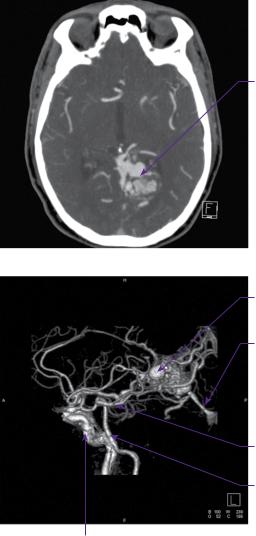
CT angiography and digital subtraction angiography (DSA) revealed that the AVM was principally supplied from the left posterior cerebral artery, with pial supply from the left anterior and middle cerebral arteries. Drainage was through a single arterialized vein into the straight sinus (Figure 22.1a–d).
(a)
Left arteriovenous malformation
(b) |
Varix within |
|
|
|
AVM |
|
Straight sinus |
Posterior cerebral artery
Basilar artery
Internal carotid artery
Figure 22.1 (a) CT angiogram axial section. There is a serpiginously-enhancing lesion in the left occipital lobe. The appearances are those of an AVM with no evidence of acute haemorrhage. (b) CT angiogram sagittal 3D reconstruction. The nidus is fed mainly by the left PCA with venous drainage into the vein of Galen. (c,d) DSA: left vertebral artery injection, anteroposterior and lateral views, respectively.
218 |
Challenging concepts in neurosurgery |
Varix within
AVM
Transverse sinus
Torcular herophili
Nidus of AVM
Straight sinus
Posterior cerebral artery
Basilar artery
Figure 22.1 Continued
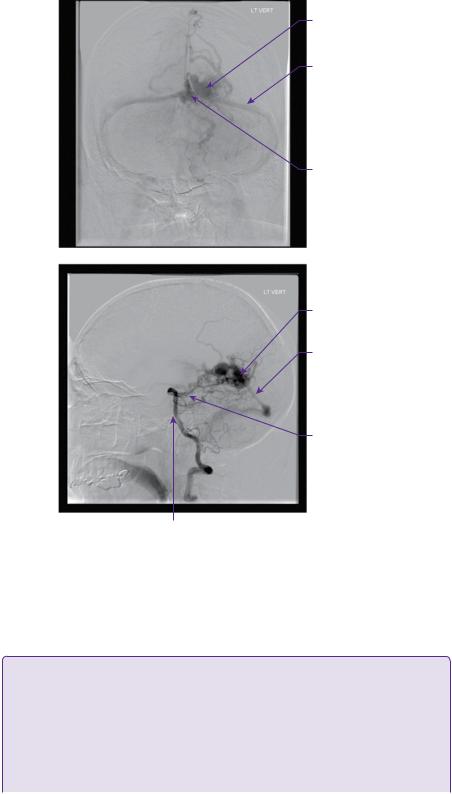
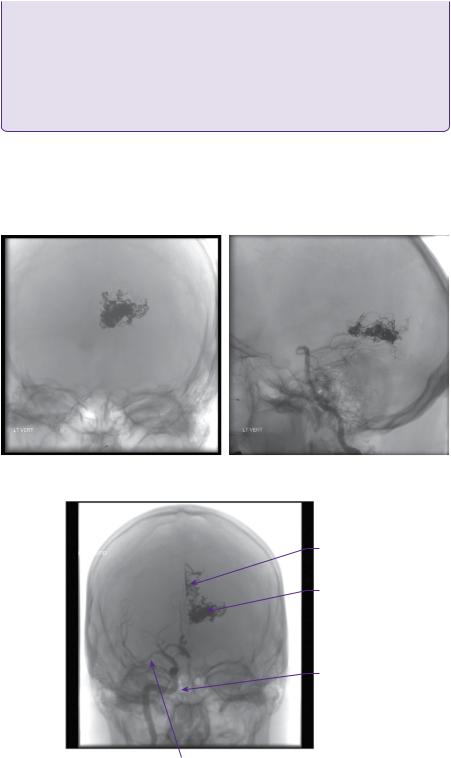
In view of the size and location of the AVM, the recommendation of the neurovascular multidisciplinary meeting was staged endovascular embolization. At the time of his first embolization, performed via internal carotid and vertebral artery catheterization, 50% of the nidus was obliterated (Figures 22.2a,b).
 Learning point Staged embolization and stereotactic radiosurgery
Learning point Staged embolization and stereotactic radiosurgery
In large lesions, which are considered to be unfavourable for surgery, staged embolization followed by
SRS has been used. Embolization has two goals:
●Targeted eradication of AVM-related aneurysms and fistulae.
●Volumetric reduction.
By reducing the size of the nidus, a larger dose of stereotactic radiation can be prescribed in order to increase the probability of nidus obliteration without increasing the risk of complications. Many
(continued)
220 Challenging concepts in neurosurgery
involve annual MRI scans as a preliminary indication of nidus obliteration. This will often require 2–3 years, but may occur up to 4 years after treatment. If there are no obvious flow voids in the area of treatment, digital subtraction angiography is indicated to confirm obliteration. Retreatment with radiosurgery is possible and would normally be recommended if obliteration has not occurred within 4 years.
 Learning point Stereotactic radiosurgery
Learning point Stereotactic radiosurgery
This is typically reserved for compact lesions, usually less than 3cm in size. It is currently the preferred treatment strategy for the majority of patients, unless there are very good clinical reasons to prefer surgery (e.g. treatment of the AVM during removal of an ICH, patient preference after careful counselling).
After treatment, which may take up to 48 months to obliterate the nidus, there is a risk of haemorrhage. Annual haemorrhage rates have been estimated at 4.8–7.9% per year for the first 2 years*, then 2.2–5% in the third, fourth, and fifth years. Notably, if the nidus is obliterated, the risk of haemorrhage is near zero. In the optimal case, i.e. small nidus, uncomplicated location, complete obliteration can be achieved in at least 90% of cases, although this decreases significantly for larger AVMs (i.e. treatment volumes of 20cm3) [4].
The technique allows a high dose of radiation to be delivered to a focal brain region, while minimizing radiation to surrounding normal brain. It is therefore ideal for centrally-located lesions, such as the brainstem, thalamus, and basal ganglia. Lim and colleagues have also demonstrated its successful
use in patients with medically intractable seizures. Furthermore, it may be used in those with multiple lesions [8], such as in familial syndromes [9,10].
*The risk of haemorrhage in the first 2 years following SRS is higher than the annual risk of haemorrhage in an untreated unruptured AVM, i.e. 2.4%.
 Expert comment Surgery for arteriovenous malformations
Expert comment Surgery for arteriovenous malformations
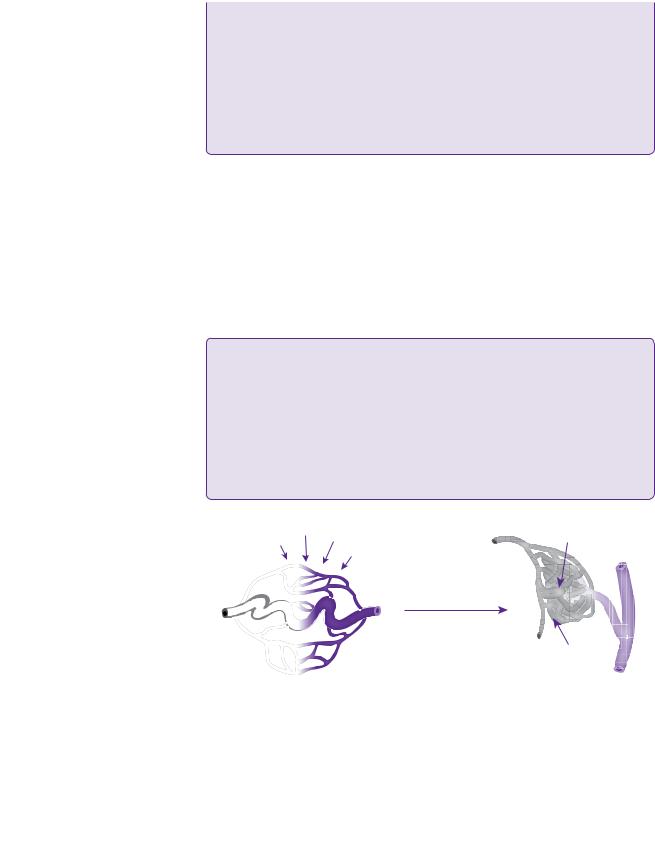
With the advent of endovascular obliteration and gamma knife radiotherapy, neurosurgical intervention is no longer the commonest modality of treatment for intracranial AVMs in most centres. The main benefit of surgery is of an immediate cure. Following dural opening, surgical technique involves delineation of the malformation, elimination of superficial feeding vessels, circumferential dissection of the nidus with control of the deep arterial pedicles and transection of the venous system. A haemosiderin or gliotic rim, or acutely haemorrhagic clot itself may provide a plane of dissection around the nidus, see figure 22.5.
It is critically important to identify arterialized veins before resection. If there is any doubt a temporary clip maybe used, as premature coagulation of a draining vein may result in catastrophic haemorrhage.
Sylvian fissure lesions are prone to en passage vessels, which must be skeletonized and preserved, with resection only of the small side branches feeding the nidus.
It is of vital importance to plan the surgical approach well in advance of surgery, using pre-operative
MRI and angiogram imaging to establish the position of probable feeding and draining vessels
 Learning point Arteriovenous malformations and driving
Learning point Arteriovenous malformations and driving
In the UK, there are very specific guidelines regarding AVMs and driving, with the diagnosis of an AVM potentially having a significant impact on the livelihood of professional drivers. Decisions are made on the background of the history and examination, e.g. incidental AVMs versus ruptured AVMs, supratentorial versus infratentorial location (Tables 22.4 and 22.5), and related seizures.
Please see the DVLA website for more information: http://www.dft.gov.uk/dvla
(continued)



 Expert comment
Expert comment  Learning point
Learning point  Expert comment
Expert comment

 Learning point
Learning point  Clinical tip
Clinical tip 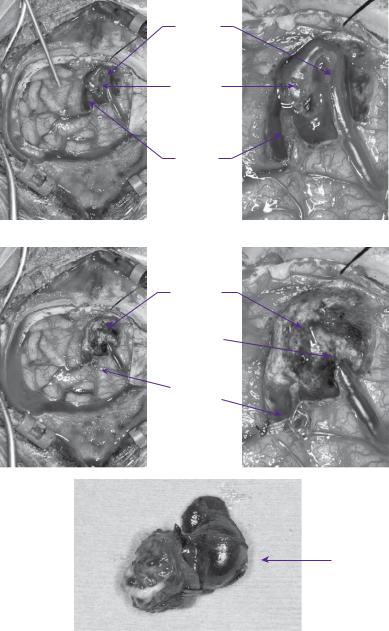
Case 22 Intracranial arteriovenous malformation |
225 |
for Spetzler–Martin grade IV and V has been reported to be 9–39% and 0–9%, respectively.
Stereotactic radiotherapy provides the least invasive treatment option. The most important factor for nidus obliteration is the dose of radiation delivered. The safe dose correlates inversely with volume, in that the larger the lesion, the smaller
Draining
vein
Nidus
of AVM
Feeding
artery
(a) |
(b) |
Resection
cavity
 Ligated vein
Ligated vein
Artery clipped
with aneurysm clip
(c) |
(d) |
Resected
AVM nidus
(e) 1cm
1cm
Figure 22.5 Intraoperative images of an occipital AVM showing cardinal anatomy (a,b) i.e. feeding artery, draining vein, and the AVM nidus. Postoperative images showing the resected AVM nidus and the residual postoperative cavity(c,d,e).
226 Challenging concepts in neurosurgery
the dose that can be given without a high risk of radionecrosis of surrounding brain. Other factors include the size of the nidus (e.g. ideally <3cm), the nidus angio-architecture (e.g. compact versus diffuse nidus), intranidal aneurysms, venous drainage, eloquent location, and previous haemorrhage. A compact nidus is a better target compared with plexiform or diffuse lesions, as they have no neural tissue inside the target volume, enabling larger does to be prescribed. It may take up to 4 years for complete obliteration of the nidus, during which time the patient continues to be at risk of haemorrhage (5% per year: see Learning point: stereotactic radiosurgery). Multiple series have been published regarding the different techniques used for radiosurgery, including proton beam, gamma knife, linear accelerator (LINAC) and CyberKnife. A recent meta-analysis of sixty-nine cohorts (twenty-two gamma knife, thirty-six LINAC) by Beijnum et al. (2011) found a 40% 2-year obliteration rate [28]. The probability of obliteration depends on the administered dose, which is influenced by the location of the AVM. Obliteration is produced by radiation-induced damage to the endothelium of the arterial wall, resulting in smooth muscle proliferation with subsequent luminal occlusion. Complications of radiosurgery include white matter oedema, seizures, radiation necrosis, and haemorrhage.
Embolization can be used as a pre-operative adjunct to surgery, leading to decreased operating times, transfusion requirements, morbidity, and mortality. As a primary modality, it offers relatively low cure rates (5–20%) with a risk of subsequent recanalization, although the use of new embolic agents, such as onyx, holds promise (15–50%). It may be offered as a primary treatment option in selected patients, i.e. for small deep-seated thalamic or basal ganglia AVMs, with one or two feeding arteries providing immediate protection against recurrent and immediate haemorrhage. Complications may be permanent or temporary, and are usually neurological deficits related to inadvertent embolization of arteries supplying healthy brain or obliteration of the venous outflow, leading to ICH. They include haemorrhage (2–5%), permanent neurological deficits (2–5%), and death (1%).
 Learning point Guidelines for treatment
Learning point Guidelines for treatment
SM I, II
●SRS.
●Microsurgery (patient preference, surgery for haematoma).
SM III
● Microsurgery/radiosurgery +/– endovascular therapy.
SM IV, V
●Observation.
●Consider tailored treatment if risk of haemorrhage/repeat.
●Bleeds.
In practice, SM grade III are the most challenging malformations to treat, representing a heterogeneous mix of pathology. This group has been subdivided into IIIA (>6cm) that are best treated with embolization and surgery, and IIIB (small, i.e. deep venous drainage and in eloquent cortex [32]) that are best treated with radiosurgery


 Expert comment
Expert comment 228 |
Challenging concepts in neurosurgery |
|
|
4. |
Mohr JP, Parides MK, Stapf C, et al. Medical management with or without interventional |
|
|
therapy for unruptured brain arteriovenous malformations (ARUBA): a multicentre, non- |
|
|
blinded, randomised trial. Lancet. 2013;383 (9917):614–621. |
|
5. |
Russin J, Spetzler R, Neurosurgery. Commentary: the ARUBA trial. Neurosurgery. 2014. |
|
|
75 (1): E96–E97 |
|
6. |
al Rodhan NR, Sundt TM, Piepgras DG, et al. Occlusive hyperaemia: a theory for the |
|
|
hemodynamic complications following resection of intracerebral arteriovenous malfor- |
|
|
mations. Journal of Neurosurgery 1993; 78 (2): 167–75. |
|
7. |
Gobin YP, Laurent A, Merienne L, et al. Treatment of brain arteriovenous malformations |
|
|
by embolization and radiosurgery. Journal of Neurosurgery 1996; 85 (1): 19–28. |
|
8. |
Lim YJ, Lee CY, Koh JS, et al. Seizure control of gamma knife radiosurgery for non- |
|
|
hemorrhagic arteriovenous malformations. Acta Neurochirurgica 2006; 99: 97–101. |
|
9. |
Kikuchi K, Kowada M, Sasajima H. Vascular malformations of the brain in hereditary |
|
|
hemorrhagic telangiectasia (Rendu-Osler-Weber disease). Surgical Neurology 1994; 41: |
|
|
374–80. |
|
10. |
Yahara K, Inagawa T, Tokuda Y, et al. [A case of multiple cerebral arteriovenous malfor- |
|
|
mations treated by gamma knife radiosurgery]. No Shinkei Geka—Neurological Surgery |
|
|
1995; 23: 1121–5. |
|
11. |
Choi JH, Mohr JP. Brain arteriovenous malformations in adults. Lancet Neurology 2005; |
|
|
4: 299–308. |
|
12. |
Hashimoto N, Nozaki K, Takagi Y, et al. Surgery of cerebral arteriovenous malforma- |
|
|
tions. Neurosurgery 2007; 61: 375–87; discussion 387–9. |
|
13. |
Nehls DG, Pittman HW. Spontaneous regression of arteriovenous malformations. |
|
|
Neurosurgery 1982; 11: 776–80. |
|
14. |
Herzig R, Burval S, Vladyka V, et al. Familial occurrence of cerebral arteriovenous |
|
|
malformation in sisters: case report and review of the literature. European Journal of |
|
|
Neurology 2000; 7 (1): 95–100. |
|
15. |
Storkebaum E, Quaegebeur A, Vikkula M, Carmeliet P. Cerebrovascular disorders: |
|
|
molecular insights and therapeutic opportunities. Nature Neuroscience. 2011;14 (11): |
|
|
1390–1397 |
|
16. |
Valavanis A. The role of angiography in the evaluation of cerebral vascular malforma- |
|
|
tions. Neuroimaging Clinics of North America 1996; 6 (3): 679–704. |
|
17. |
Hofmeister C, Stapf C, Hartmann A, et al. Demographic, morphological, and clinical |
|
|
characteristics of 1289 patients with brain arteriovenous malformation. Stroke 2000; 31: |
|
|
1307–10. |
|
18. |
Hoh BL, Chapman PH, Loeffler JS, et al. Results of multimodality treatment for 141 |
|
|
patients with brain arteriovenous malformations and seizures: factors associated with |
|
|
seizure incidence and seizure outcomes. Neurosurgery 2002; 51: 303–9; discussion |
|
|
309–11. |
|
19. |
Yeh HS, Kashiwagi S, Tew JM, Jr, et al. Surgical management of epilepsy associated with |
|
|
cerebral arteriovenous malformations. Journal of Neurosurgery 1990; 72: 216–23. |
|
20. |
Trussart V, Berry I, Manelfe C, et al. Epileptogenic cerebral vascular malformations and |
|
|
MRI. Journal of neuroradiology.\ Journal de Neuroradiologie 1989; 16: 273–84. |
|
21. |
Yeh HS, Privitera MD. Secondary epileptogenesis in cerebral arteriovenous malforma- |
|
|
tions. Archives of Neurology 1991; 48: 1122–4. |
|
22. |
Heikkinen ER, Konnov B, Melnikov L, et al. Relief of epilepsy by radiosurgery of cerebral |
|
|
arteriovenous malformations. Stereotactic & Functional Neurosurgery 1989; 53 (3): |
|
|
157–66. |
|
23. |
Lv X, Li Y, Jiang C, et al. Brain arteriovenous malformations and endovascular treat- |
|
|
ment: effect on seizures. Interventional Neuroradiology 2010; 16: 39–45. |
|
24. |
Hernesniemi JA, Dashti R, Juvela S, et al. Natural history of brain arteriovenous malfor- |
|
|
mations: a long-term follow-up study of risk of hemorrhage in 238 patients. Neurosurgery |
|
|
2008; 63: 823–9; discussion 829–31. |
Case 22 Intracranial arteriovenous malformation |
229 |
25.Stapf C, Mast H, Sciacca RR, et al. Predictors of hemorrhage in patients with untreated brain arteriovenous malformation. Neurology 2006; 66: 1350–5.
26.Ondra SL, Troupp H, George ED, et al. The natural history of symptomatic arteriovenous malformations of the brain: a 24-year follow-up assessment. Journal of Neurosurgery 1990; 73 (3): 387–91.
27.Pollock BE, Flickinger JC, Lunsford LD, et al. Factors that predict the bleeding risk of cerebral arteriovenous malformations. Stroke 1996; 27: 1–6.
28.van Beijnum J, van der Worp HB, Buis D, et al. Treatment of brain arteriovenous malformations: a systematic review and meta-analysis. Journal of the American Medical Association 2011; 306 (18): 2011–19.
29.Spetzler RF, Wilson CB, Weinstein P, et al. Normal perfusion pressure breakthrough theory. Clinical Neurosurgery 1978; 25: 651–72.
30.Spetzler RF, Hargraves RW, McCormick PW, et al. Relationship of perfusion pressure and size to risk of hemorrhage from arteriovenous malformations. Journal of Neurosurgery 1992; 76 (6): 918–23.
31.Turjman F, Massoud TF, Vinuela F, et al. Correlation of the angioarchitectural features of cerebral arteriovenous malformations with clinical presentation of hemorrhage. Neurosurgery 1995; 37: 856–60; discussion 860–2.
32.de Oliveira E, Tedeschi H, Raso J. Comprehensive management of arteriovenous malformations. Neurological Research 1998; 20 (8): 673–83.
33.Menghini VV, Brown RD, Jr, Sicks JD, et al. Clinical manifestations and survival rates among patients with saccular intracranial aneurysms: population-based study in Olmsted County, Minnesota, 1965 to 1995. Neurosurgery 2001; 49: 251–6; discussion 256–8.