


Intrahepatic Bile Ducts
56
2 Intrahepatic Bile Ducts
2.1 Normal Anatomy and Variants
#26 Normal Anatomy
KEY FACTS: ANATOMY
●The bile ducts generally follow the internal hepatic segmental anatomy (Fig.26a). However,marked variation in the branching pattern is common
●Major branches:
–Right hepatic duct, dividing into the posterior right hepatic duct (dorsocaudal course) and the anterior right hepatic duct (ventrocranial course)
–Left hepatic duct (more anterior in position)
●Segmental branches:
–From the posterior right hepatic duct: right posterior superior duct (serves segment VII) and right posterior inferior duct (segment VI)
–From the anterior right hepatic duct: right anterior superior duct (segment VIII) and right anterior inferior duct (segment V)
–The ductal branches that serve segments I–IV stem directly from the left hepatic duct
●Projective MRCP nearly invariably shows the right and left hepatic ducts and their major branches (Reinhold and Bret 1996; Fig. 26b)
●Heavily T2-weighted cross-sectional images also show smaller branches throughout the liver parenchyma (complete absence of bile ducts in a lobe or segment is abnormal)
●The degree of visualization of small and/or peripheral branches depends on the following:
–Technical parameters (e.g., projective versus cross-sectional, choice of slice thickness)
–Patient-related parameters (age, constitution)
References
Dodd GD III (1993) An American’s guide to Couinaud’s numbering system. AJR Am J Roentgenol 574–575
Reinhold C, Bret PM (1996) Current status of MR cholangiopancreatography. AJR Am J Roentgenol 166 :1285–1295
Taylor AJ, Bohorfoush AG (1997) Interpretation of ERCP. Lippincott-Raven, Philadelphia, p 62
2 Intrahepatic Bile Ducts |
57 |
Fig. 26. a The intrahepatic biliary tree and its relation to the hepatic segments. Note that the distal portions of the right and left hepatic duct travel outside the liver substance before they join to form the common hepatic duct. The right posterior hepatic duct serves segments VI and VII and runs in a more horizontal direction than the right anterior duct. (Reprinted with permission from Taylor and Bohorfoush 1997) b Projective image obtained in a young asymptomatic patient showing the common hepatic duct (C)
and right (R) and left (L) hepatic duct as well as the posterior (P) and anterior (A) right hepatic ducts
a
b
58 2.1 Normal Anatomy and Variants
#27 Variant Anatomy (1):
Variable Junction of the
Posterior Right Hepatic Duct
Related topic: #52 (after cholecystectomy: stricture/transection of aberrant bile duct)
KEY FACTS: ANATOMY
●Aberrant bile ducts occur in 14%–28% of the population (Sussman et al. 1986)
●The most common anomaly is a failure of fusion of the anterior and posterior right segmental ducts. In the majority of cases, the right posterior segmental duct joins the left hepatic duct (Fig. 27a, b; see also Fig. 63). This appears as a trifurcation if the right posterior duct joins the left hepatic duct near the confluence with the right anterior duct
●In 2%–3% of the population, the right posterior hepatic duct drains into the common hepatic duct, cystic duct, gallbladder, common bile duct, or even duodenum (Fig. 27a, c)
●Clinical significance: risk of operative bile duct injury, particularly during (laparoscopic) cholecystectomy (see #52)
References
Russell E, Yrizzary KM, Montalvo BM et al. (1990) Left hepatic duct anatomy: implications. Radiology 174 : 353–356
Sussman SK, Hall FM, Elboim CM (1986) Radiographic assessment of anomalous bile ducts. Gastrointest Radiol 11: 269–272
Taourel P, Bret P, Reinhold C, Barkum AN, Atri M (1996) Anatomic variants of the biliary tree: diagnosis with MRCP. Radiology 199 : 521–527
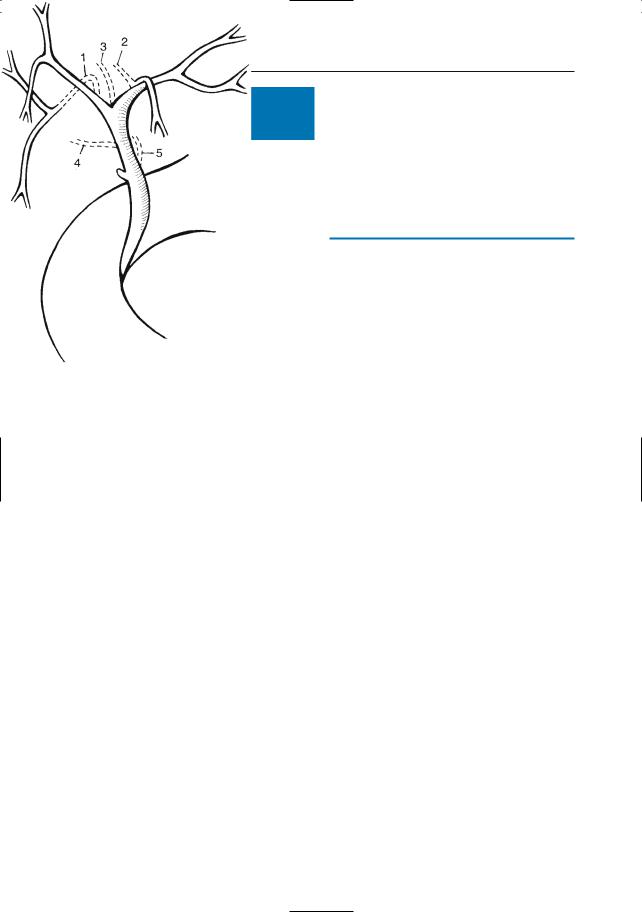
Fig. 27. a Variations in the drainage pattern of the right posterior hepatic duct: drainage into right anterior duct (1), left hepatic duct (2), bifurcation (3), lateral side of common hepatic duct (4), and medial side of common hepatic duct (5). (Reprinted with permission from Russell et al. 1990)
2 Intrahepatic Bile Ducts |
59 |
b |
c |
d |
e |
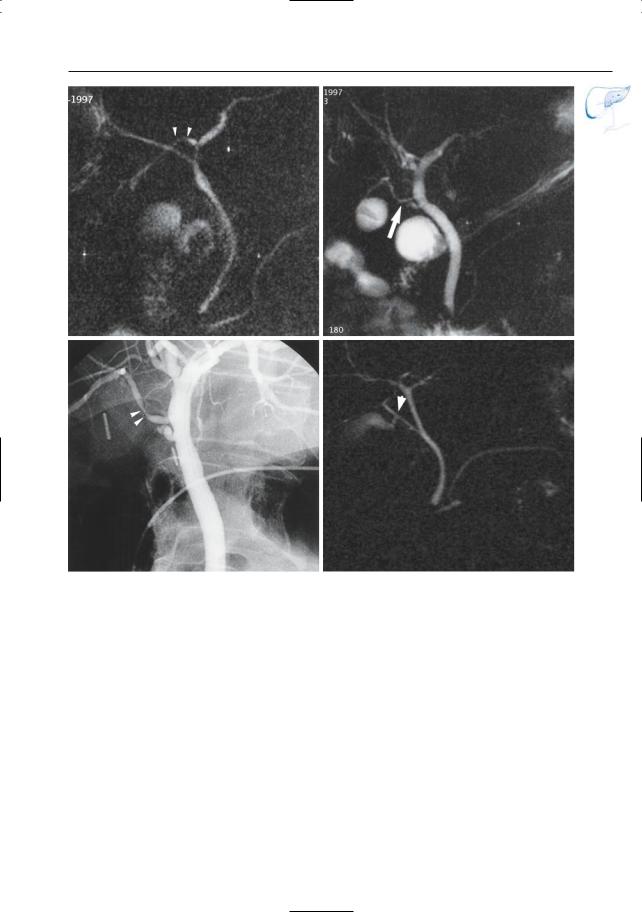
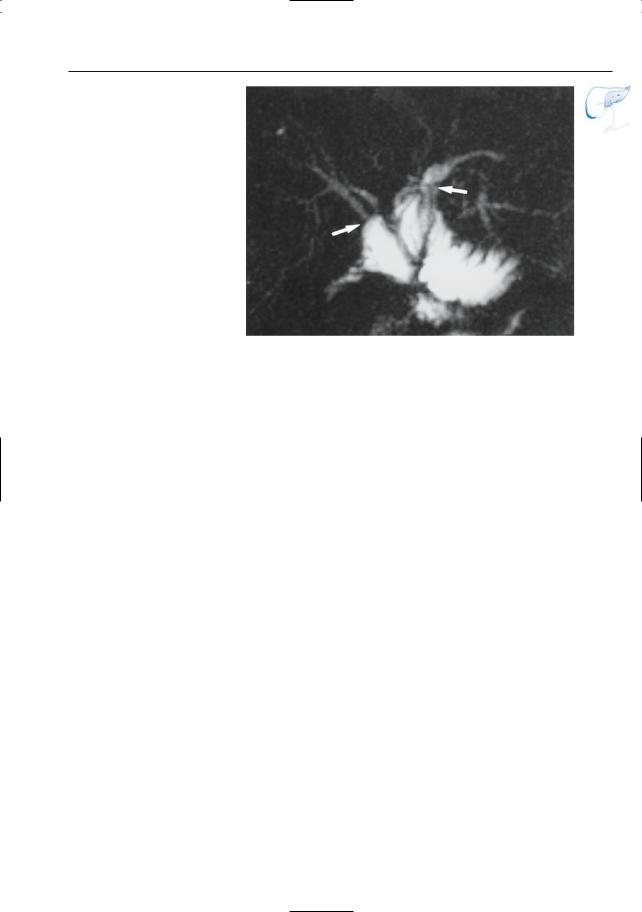
Fig. 27. b Projective image showing drainage of the right posterior segmental duct into the left hepatic duct (arrowheads). c, d In another patient, projective MR image (c) showing aberrant right posterior duct draining into the common hepatic duct in close proximity to the cystic duct (arrow). d Corresponding ERCP image confirms the presence of an aberrant
right posterior hepatic duct. Moreover, it shows a short stenosis of this duct (arrowheads), probably related to trauma during cholecystectomy. Note that this stenosis is not well seen in c (see #23). e Different patient. Projective MR (RARE) image showing aberrant right posterior segmental duct; the cystic duct appears to drain in this duct (arrow)

60 2.1 Normal Anatomy and Variants
#28 Variant Anatomy (2):
Other Variations
KEY FACTS: ANATOMY
●Many other variations in anatomy and branching pattern exist, including the following:
–Quadrifurcation of the right or main hepatic duct (Fig. 28a, b)
–Cystohepatic duct: intrahepatic ducts draining into the gallbladder (Fig. 28c)
–Subvesicle ducts (also called Luschka ducts, found in 35% of autopsy cases): tiny ducts (<2 mm in size) beginning in the wall of the gallbladder but not communicating with the lumen
–Unusually large right or left segmental branches
References
Schulte S (1995) Embryology and congenital anomalies of the bile and pancreatic ducts. In: Silvis S, Rohrmann C, Ansel H (eds) Endoscopic retrograde cholangiopancreatography. IgakuShoin, New York, pp 114–126

2 Intrahepatic Bile Ducts |
61 |
a
Fig. 28. Projective MR images showing a quadrifurcation of the right hepatic duct (arrow), b quadrifurcation of the main hepatic duct (arrow), and c hepatocystic duct (arrows)
b
c
62 2.1 Normal Anatomy and Variants
#29 Postoperative Anatomy:
After Hepat(ic)ojejunostomy
Related topics: #49 (after hepaticojejunostomy: anastomotic stricture), #56 (recurrent tumor after hepaticojejunostomy), #66 (postoperative anatomy: after the Whipple procedure)
KEY FACTS: TECHNIQUE
●Hepat(ic)ojejunostomy: subtype of bilioenteric anastomoses
●Indications: neoplasms located in the liver hilum or common hepatic duct, benign strictures of common hepatic duct, etc.
●Terminology (Karakousis and Douglass 1977):
–Hepatojejunostomy in the strict sense of the term: anastomosis between the liver hilum and jejunum (operation performed when individual ducts can not be anastomosed to the jejunum)
–Hepaticojejunostomy: duct-to-mucosa anastomosis with main hepatic duct or with left and/or right hepatic duct
–Intrahepatic cholangiojejunostomy: anastomosis with more peripheral bile duct
●Common reasons for investigating the patency of bilioenteric anastomoses: fever, abnormal liver function, jaundice
●Complications: anastomotic stricture, cholangitis, biliary stones, recurrent tumor (see #49, 56)
KEY FACTS: MRI
●MR cholangiography shows the size of intrahepatic bile ducts and dimensions of anastomosis (Fig. 29; Pavone et al. 1997)
●MR criteria for a normal anastomosis:
–The anastomosis should be visible (i.e., filled with fluid) but should not necessarily have the same diameter as the proximal bile duct
–No significant intrahepatic bile duct dilation
●Note: Administration of oral contrast medium (e.g., tap water) and spasmolytic agent (see # 14) required
References
Karakousis CP, Douglass HO (1977) Hilar hepatojejunostomy in resection of carcinoma of the main hepatic duct junction. Surg Gynecol Obstet 145 : 245–248
Bengmark S, Ekberg H, Evander A, Klofver-Stahl B, Tranberg KG (1988) Major liver resection for hilar cholangiocarcinoma. Ann Surg 207 : 120–125
Pavone P, Laghi A, Catalano C et al. (1997) MR cholangiography in the examination of patients with biliary-enteric anastomoses. AJR Am J Roentgenol 169 : 807–811
2 Intrahepatic Bile Ducts |
63 |
Fig. 29. Patient who underwent resection of the common hepatic duct and separate left and right hepaticojejunostomy. Both anastomoses are well seen on this projective image (arrows)