

1 MRCP Technique |
27 |
1.2 Practical Setup of an MRCP Study
#11 Selection of Slice Location
for Projective MRCP
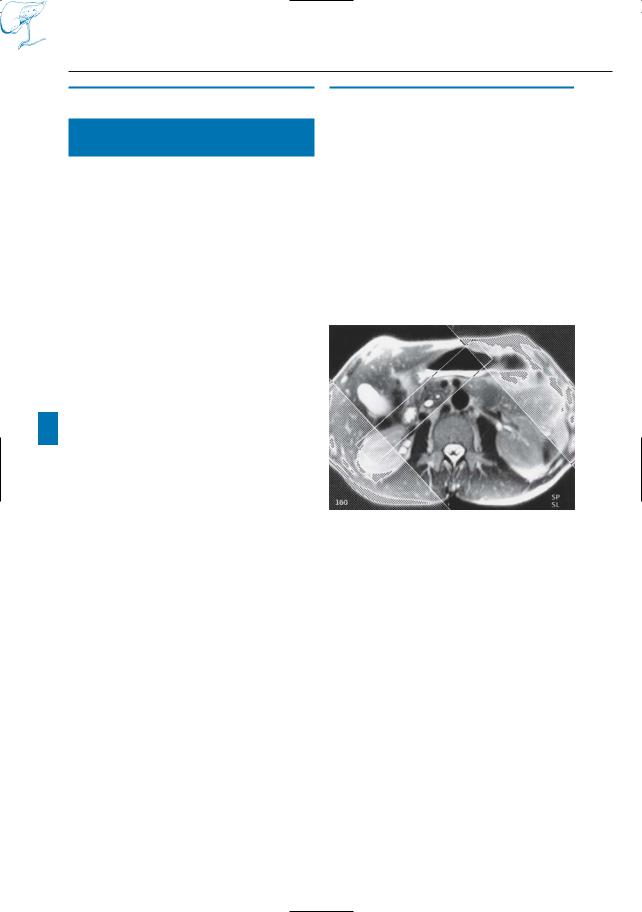
METHOD (FIG. 11)
●Cross-sectional T2-weighted MR images are obtained first
●Projective imaging is obtained in the plane determined by the position of the structures of interest (e.g., bile duct, pancreatic duct) as seen on the crosssectional images
●Superimpositions of bowel contents can be eliminated by varying the slice orientation and adjusting the slice thickness
●Several (up to ten to 15) views should usually be obtained in order to obtain all the relevant information
!● Note: The selection of the optimal section planes for projective MRCP requires a preliminary study of cross-sectional images. Preferably, both axial and coronal images (e.g., snapshot T1 and dou- ble-echo snapshot T2) should be routinely obtained and analyzed. One could call this approach “real-time interactive MRCP”.
References
Laubenberger J, Büchert M, Schneider B, Blum B, Hennig J, Langer M (1995) Breath-hold projection magnetic resonance cholangio-pancreatico- graphy (MRCP): a new method for the examination of the bile and pancreatic ducts. Magn Reson Med 33 : 18–23
Van Hoe L, Gryspeerdt S, Vanbeckevoort D et al. (1998) Normal Vaterian sphincter complex: evaluation of morphology and contractility with dynamic single-shot MR cholangiography. AJR 170 : 1497–1500
Fig. 11. Axial cross-sectional T2-weighted MR image used to select the optimal section plane for projective MRCP. Saturation bands are used to avoid infolding
28 1.2 Practical Setup of an MRCP Study
#12 Selection of Slice Thickness
KEY FACTS
●Cross-sectional techniques: slice thickness usually 5–7 mm, representing an optimal compromise between:
–Signal-to-noise ratio (increases as the slice thickness increases)
–Contrast resolution (decreases as the slice thickness increases)
●Note: Snapshot T2-weighted images are preferentially obtained in an interleaved fashion, i.e., two separate series of images are obtained with an intersection gap equal to the slice thickness (to reduce artifact related to cross talk; Bosmans et al. 1997)
●Projective MRI:
–Use of a slice thickness of 3 cm constitutes a good compromise between examination volume and contrast resolution (Fig. 12)
–A slice thickness of 2 cm may be optimal for particular studies (e.g., vaterian sphincter complex, ductal anatomy in children)
–A larger slice thickness (up to 12 cm) may be selected to obtain “overview” images; however, small structures and lesions may become invisible
References
Bosmans H, Van Hoe L, Gryspeerdt S, Kiefer B, Van Steenbergen W, Baert AL, Marchal G (1997) Technical note. Single-shot T2-weighted MR imaging of the upper abdomen: preliminary experience with the double echo HASTE technique. AJR Am J Roentgenol 169 : 1291–1293
Laubenberger J, Büchert M, Schneider B, Blum B, Hennig J, Langer M (1995) Breath-hold projection magnetic resonance cholangio-pancre- aticography (MRCP): a new method for the examination of the bile and pancreatic ducts. Magn Reson Med 33 : 18–23
Reuther G, Kiefer B, Tuchmann A (1996) Cholangiography before biliary surgery: single-shot MR cholangiography versus intravenous cholangiography. Radiology 198 : 561–566
1 MRCP Technique |
29 |
|
a
Fig. 12 a–c. Projective images obtained with slice thicknesses of a 5 cm, b 3 cm, and c 1 cm. The quality of the images shown in a and b is nearly equivalent. However, the small intrahepatic duct shown in b (arrowheads) is somewhat less sharply defined in a, probably as a result of volume averaging. In c, the intrahepatic branches are not seen because they are not within the section
b
c
30 1.2 Practical Setup of an MRCP Study
#13 Dynamic Evaluation of the
Vaterian Sphincter Complex
KEY FACTS
●Rationale (see also # 120):
–A normal sphincter contracts approximately four times per min
–On MR images, the appearance of the vaterian sphincter complex varies: during contraction,it is not visualized (no fluid in lumen); during relaxation, it is seen as a thin, fluid-containing structure
–Dynamic imaging of the vaterian sphincter complex allows both anatomy and contractility to be evaluated
●Technique (Van Hoe et al. 1998):
–Localization of the distalmost portions of the common bile duct and pancreatic duct on cross-sectional images
–Selection of optimal slice position and orientation (showing the distal parts of the common bile duct and pancreatic duct; see # 11)
–Repetitive imaging of the same section during consecutive (up to 20) episodes of breathholding
References
Van Hoe L, Gryspeerdt S, Vanbeckevoort D et al. (1998) Normal Vaterian sphincter complex: evaluation of morphology and contractility with dynamic single-shot MR cholangiography. AJR 170 : 1497–1500
1 MRCP Technique |
31 |
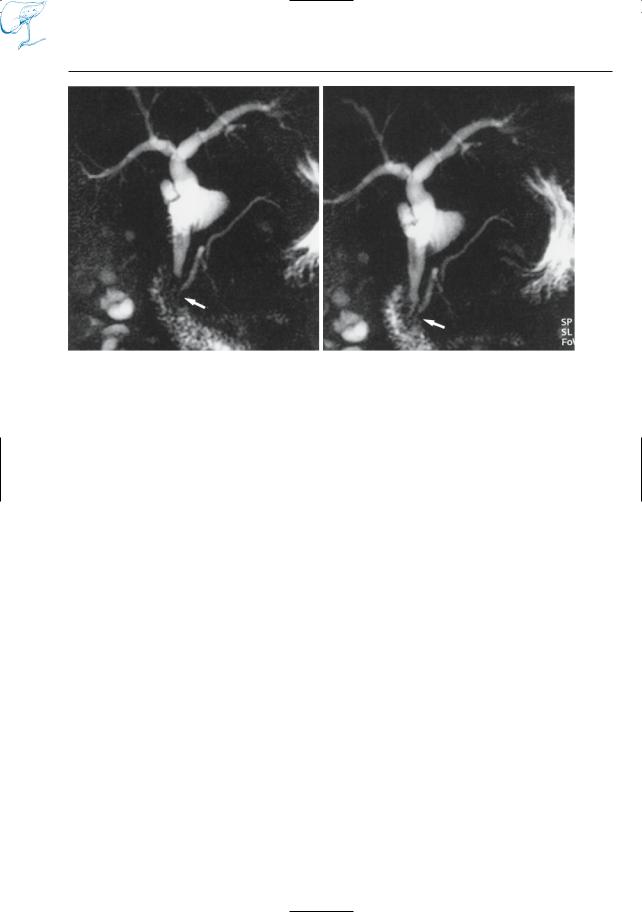
a
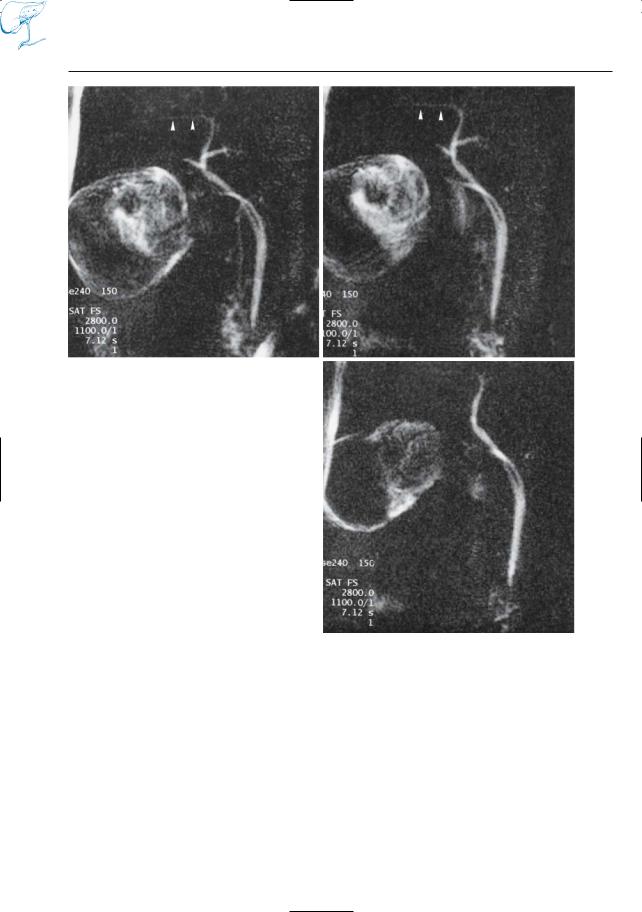
Fig. 13 a, b. Two images from a dynamic study of the vaterian sphincter complex, obtained at the same location at an interval of ± 10 s. Note that the distal (intramural) parts of the common bile duct
b
and pancreatic duct are not visible in a (image obtained during contraction of the sphincter), while they are clearly visible in b (arrows). For further details, see # 120