


Gallbladder and Cystic Duct
194
4 Gallbladder and Cystic Duct
4.1 Normal Anatomy and Variants
# 92 Gallbladder
KEY FACTS: ANATOMY (GORE ET AL. 1994)
●The gallbladder is located in a fossa on the lower surface of the liver between the right and left lobes
●Normal wall thickness: < 2–3 mm
●Divided into four parts: fundus, body, infundibulum, and neck
KEY FACTS: VARIANTS
●Location (e.g.,may be intrahepatic,suprahepatic, retroperitoneal)
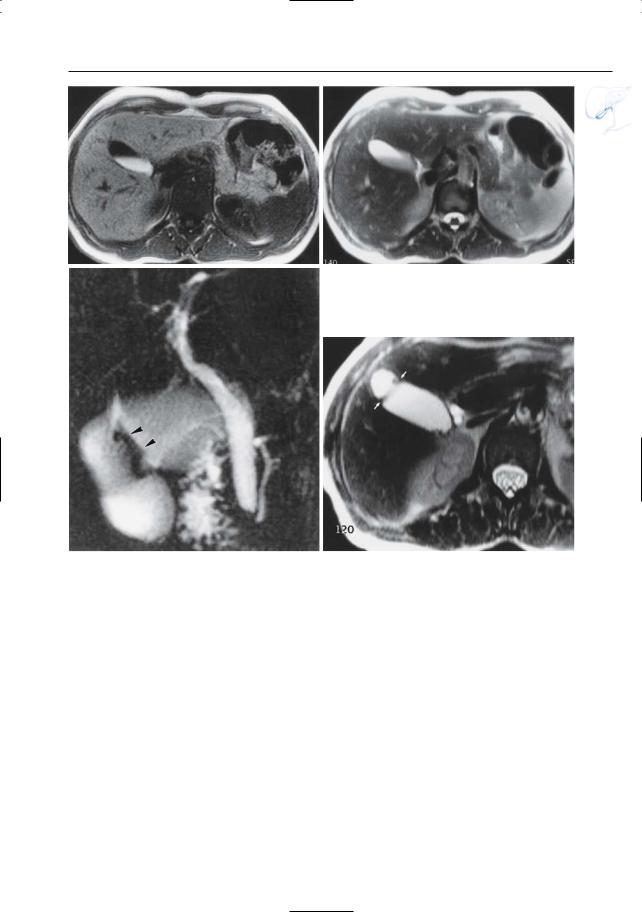
●Content: sludge (calcium bilirubinate granules and cholesterol crystals), commonly found during prolonged fasting and hyperalimentation (Fig. 92a, b)
●Classification of septa:
–Longitudinal septum (= duplication; 1 in 3000 to 1 in 12000);
–Isolated transverse septum
–Phrygian cap: 2%–6% of population, kinking/folding of fundus and sometimes septum; Fig. 92c, d)
●Size (“cholecystomegaly” vs. “microgallbladder”)
KEY FACTS: MRI (BRET AND REINHOLD 1997)
●Signal intensity of gallbladder content:
–T2: hyperintense
–T1: variable, depending on the composition and concentration of bile (higher signal intensity in patients fasting for several hours; Demas et al. 1985)
●The normal gallbladder wall is thin and hypointense relative to retroperitoneal fat on non-fat-suppressed snapshot T2weighted MR images
●Signal intensity of sludge (Fig. 92a, b):
–T1: hyperintense
–T2: slightly hypointense (differential diagnosis with stones: shape)
References
Bret P, Reinhold C (1997) MRI of the gallbladder. In: Rossi P (ed) Biliary tract radiology. Springer, Berlin Heidelberg New York, pp 59–69
Demas BE, Hricak H, Moseley M et al. (1985) Gallbladder bile: an experimental study in dogs using MR imaging and proton MR spectroscopy. Radiology 157 : 453–455
Freeny PC, Stevenson GW (1994) Margulis and Burhenne’s alimentary tract Radiology, 5th edn. Mosby, St Louis
Gore RM, Ghahremani GG, Fernbach SK (1994) Gallbladder: anomalies and anatomic variants. In: Gore RM, Levine MS, Laufer I (eds) Textbook of gastrointestinal radiology. Saunders, Philadelphia, pp 1621–1635
Hakansson K, Christoffersson JO, Leander P et al. (2002) On the appearance of bile in clinical MR cholangiopancreatography. Acta Radiol 43 : 401– 410
4 Gallbladder and Cystic Duct 195
a |
b |
c |
d |
Fig. 92 a, b. Sludge. a T1and b T2-weighted images showing sludge in dependent portion of the gallbladder. c, d Phrygian cap. c Projective image showing folding of fundus with larger diameter of
the distal part and presence of a septum (arrowheads). d Axial T2-weighted image showing septum (arrows). Note higher signal intensity of bile within the fundus
196 4.1 Normal Anatomy and Variants
#93 Cystic Duct
Related topics: #27, 28 (intrahepatic bile ducts, variant anatomy), #82, 83 (extrahepatic duct, complications after cholecystectomy)
KEY FACTS: ANATOMY
●Average diameter: 1.8 mm
●Average length: 2–4 cm
●Course: classically serpiginous with tight S-shaped bends
●Location:
–Distal part usually posterior to the common bile duct (95%)
–May run parallel to the common hepatic duct for a short distance
–In 10%, the two ducts have a long parallel course
●Insertion: the point at which the cystic duct joins the bile duct is quite variable (Shaw et al. 1993) (Fig. 93a):
–Upper part of bile duct (including left or right hepatic duct): ± 30%
–Middle part: ± 60%
–Lower part: ± 10%
KEY FACTS: MRI
●Small,tubular fluid-containing structure between the gallbladder and bile duct
●Usually easily recognized due to its characteristic location and “folded” appearance
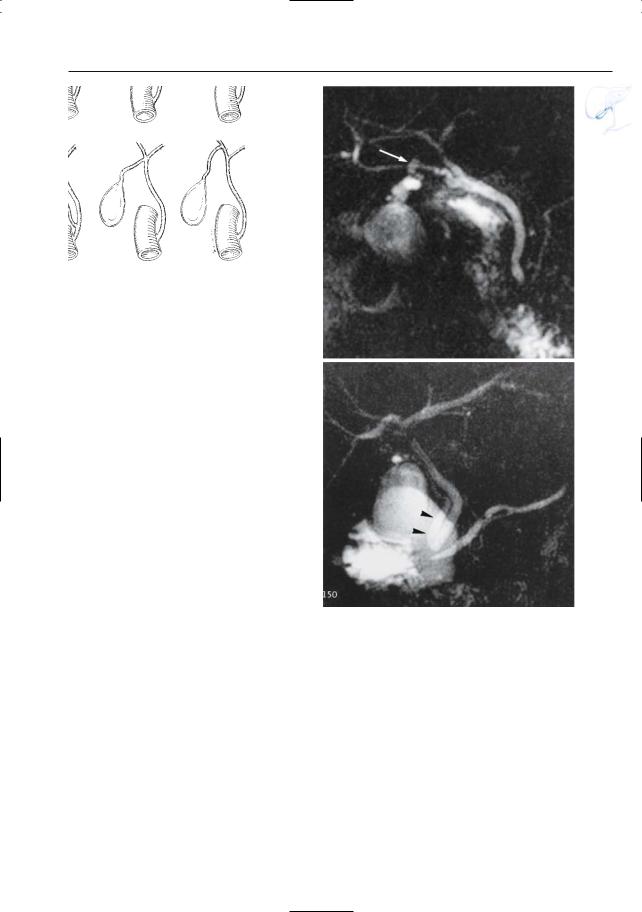
●Identification of anatomic variants (high and low insertion, long parallel course) is important if (laparoscopic) cholecystectomy is planned (see #52, 82, 83) (Fig. 93b, c)
References
Schulte SJ (1994) Embryology, normal variation, and congenital anomalies of the gallbladder and biliary tract. In: Freeny PC, Stevenson GW (eds) Marqulis and Burhenne’s alimentary tract radiology. Mosby, St. Louis, pp 1251–1274
Shaw MJ, Dorscher PJ, Vennes JA (1993) Cystic duct anatomy: an endoscopic perspective. Am J Gastroenterol 88 : 2102–2106
Silvis SE (1995) The normal bile duct. In: Silvis S, Rohrmann C, Ansel H (eds) Endoscopic retrograde cholangiopancreatography. Igaku-Shoin, New York, pp 168–192
Turner MA, Fulcher AS (2001) The cystic duct: normal anatomy and disease processes. Radiographics 21 : 3–22
4 Gallbladder and Cystic Duct 197
a |
b |
Fig. 93. a Variations in the insertion of the cystic |
|
duct. 1, “classical lateral insertion; 2, long parallel |
|
course; 3, medial (spiral) insertion; 4, low insertion; |
|
5, insertion at bifurcation; 6, in right hepatic duct. |
|
(From Schulte S.J. 1994, with permission). b Projec- |
|
tive MR image showing high insertion of the cystic |
|
duct in an aberrant right hepatic duct (arrow). |
|
c Projective MR image showing extremely low inser- |
|
tion of the cystic duct (arrowheads), near the vate- |
c |
rian sphincter complex |
|