

6 Pancreatic Ducts 375
6.4Malignant Tumors and Tumors with Malignant Potential
#185 Adenocarcinoma, General
KEY FACTS: DISEASE
●Fourth to fifth leading cause of cancer death in the United States
●Incidence in autopsy series: 2%
●Age peak: seventh decade
●Resectable at presentation: 8%–15%
●CA 19-9 increased in 80%–90%
●Origin:
–Exocrine ductal epithelium: 99%
–Acinar portion of the pancreatic gland: 1%
●Extent (Cubilla et al. 1979)
–65% of patients have advanced local disease or distant metastases
–21% have local disease with spread to regional lymph nodes
–14% have tumor confined to the pancreas
●Metastases
–Liver: 30%–60%
–Regional lymph nodes: 15%–28%
–Peritoneum: 7%–10%
–Other sites: e.g., lung, pleura, bone
●Symptoms:
–Epigastric pain radiating to the back
–Obstructive jaundice
–New-onset diabetes, steatorrhea
●Five-year survival rate: 1%–5%
References
Cubilla AL, Fitzgerald PJ (1979) Cancer of the pancreas (nonendocrine): a suggested morphological classification. Semin Oncol 6 : 285–297
Warshaw AL, Fernandez-del Castillo C (1992) Pancreatic carcinoma. New Engl J Med 326 : 455–465
376 6.4 Malignant Tumors and Tumors with Malignant Potential
#186 Adenocarcinoma,
Signal Intensity
KEY FACTS: MRI
●Signal intensity:
–Nearly invariably hypointense on T1-weighted magnetization-prepared snapshot gradient echo images (see #9)
–May be isointense, however, if the surrounding pancreatic tissue is abnormal (pancreatitis)
–Isoor hyperintense on T2-weighted images
–Usually hypointense on contrast-en- hanced scans
●Technical remarks about contrast-en- hanced scans:
–Rapid bolus injection is mandatory
–Timing is important: imaging should
be done in the pancreatic phase (± 40 s after injection)
● Note: Value of sequences: |
|
|
|
|
! |
||
– |
T1 much better than T2 for tumor |
||
|
detection |
|
|
– |
Magnetization-prepared |
snapshot |
|
|
gradient echo particularly reliable |
||
– Contrast-enhanced scans |
often re- |
||
|
quired for preoperative evaluation (as- |
||
|
sessment of vascular anatomy, detec- |
||
|
tion of lymph node metastases) |
||
References
Gabata T,Matsui O,Kadoya M et al. (1994) Small pancreatic adenocarcinomas: efficacy of MR imaging with fat suppression and gadolinium enhancement. Radiology 193 : 683–688
Ichikawa T, Haradome H, Hachiya J et al. (1997) Pancreatic ductal adenocarcinoma: preoperative assessment with helical CT versus dynamic MR imaging. Radiology 202 : 655–662
Kelekis NL, Semelka RC (1997) MRI of pancreatic tumors. Eur Radiol 7 : 875–886
6 Pancreatic Ducts 377
a |
b |
c |
d |
e |
f |
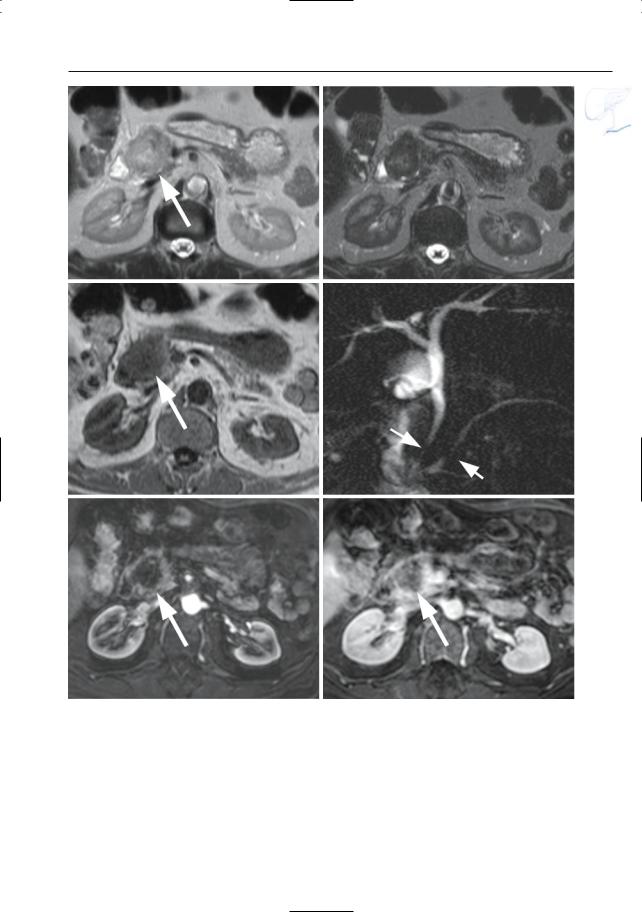
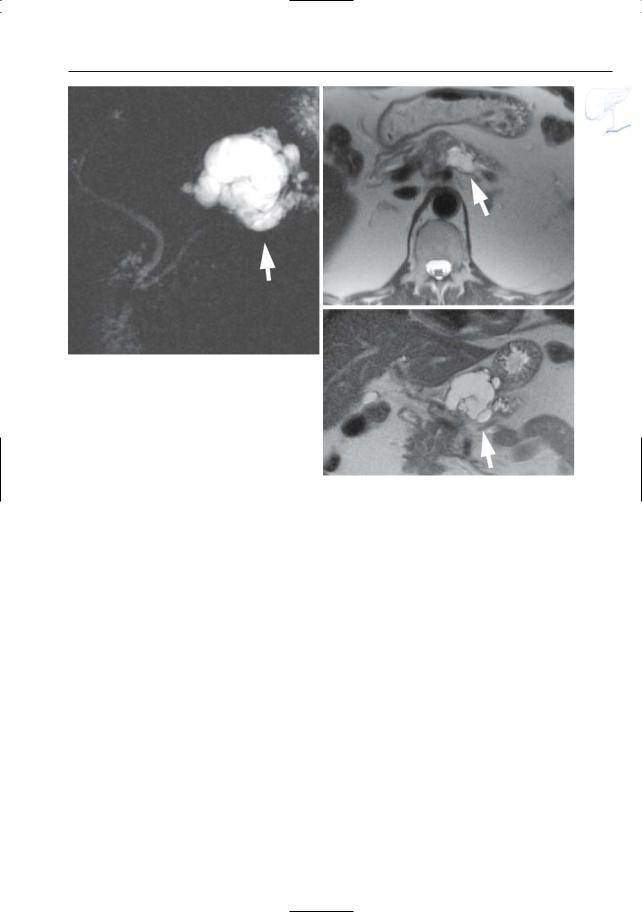
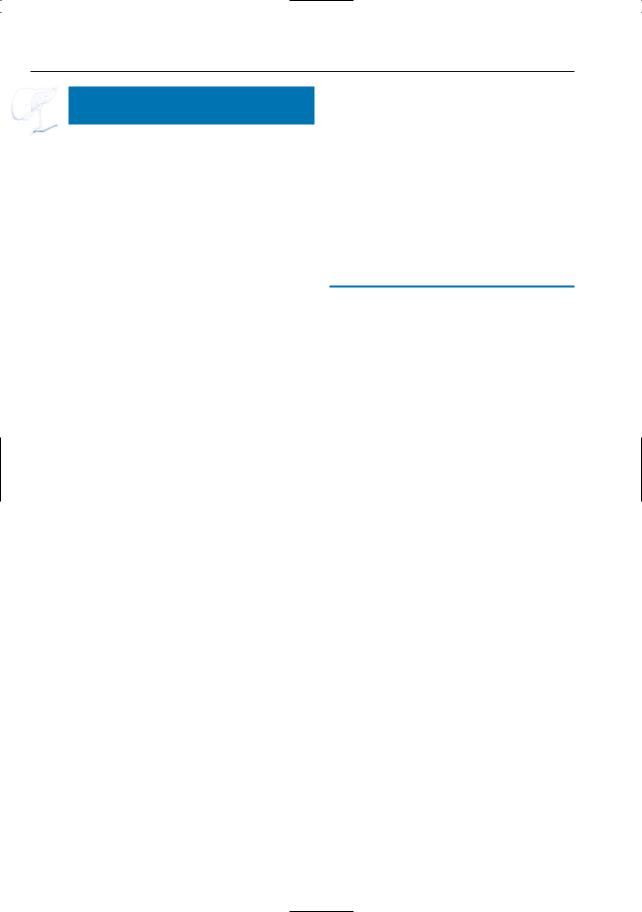
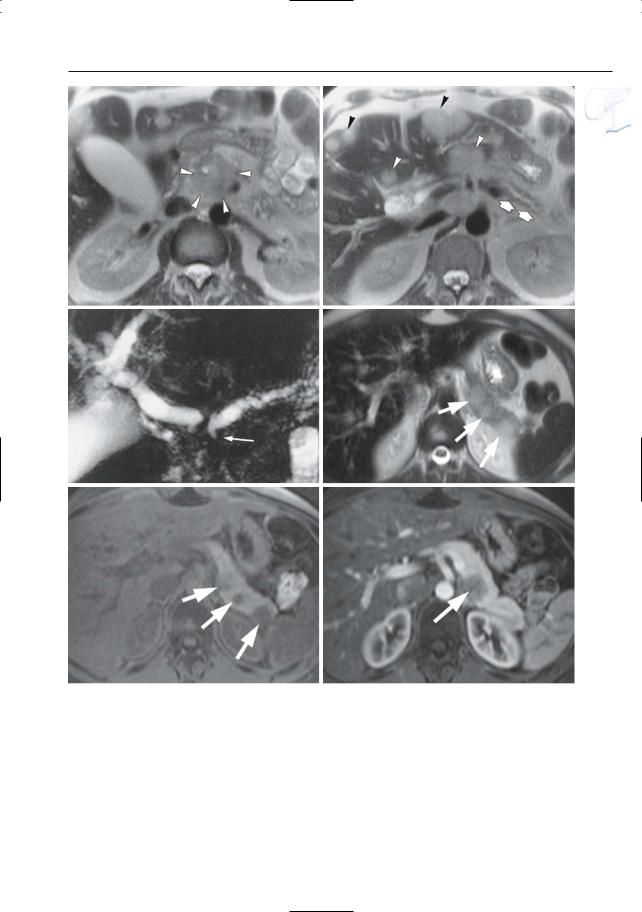
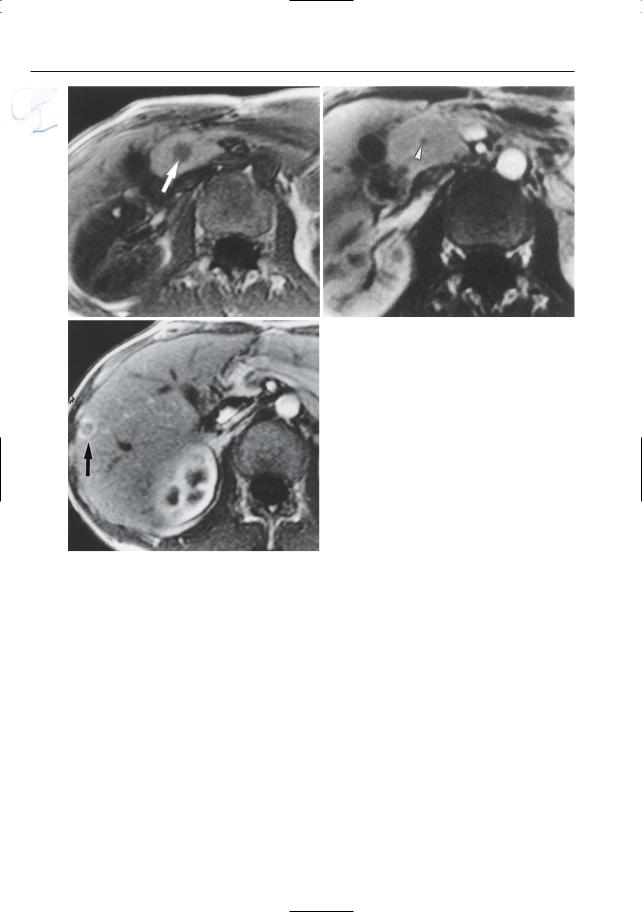
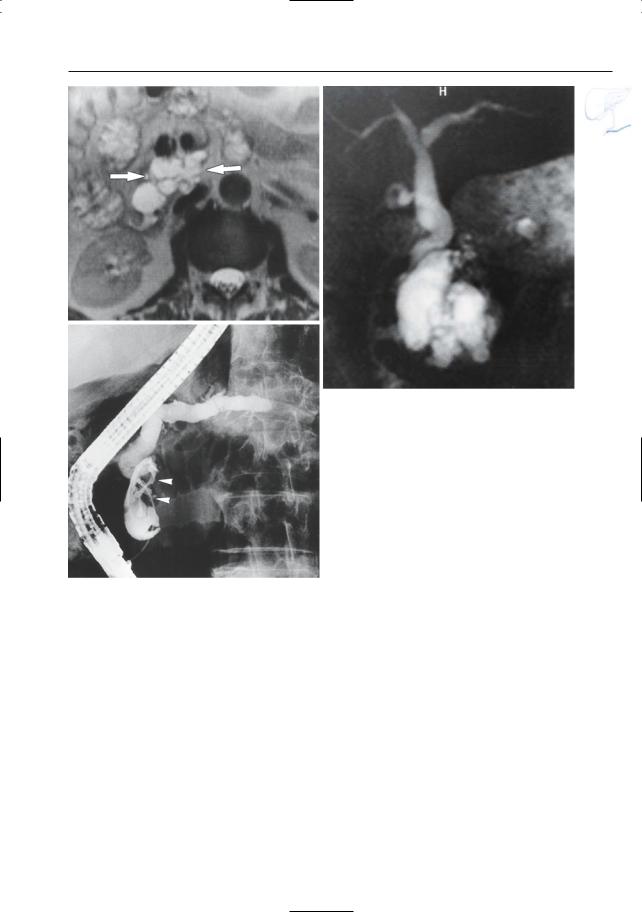
Fig. 186 a–f. Axial T2-weighted HASTE images (TE 60 and 360) (a, b) and (c) axial T1-weighted image showing a focal lesion in pancreatic head (arrows): adenocarcinoma. The lesion is markedly hypointense to normal pancreatic tissue on the T1weighted image. d Projective image showing focal narrowing of the distal common bile duct and pancreatic duct,approximately at the same level (double
duct sign) (arrows). Note nearly normal size of proximal pancreatic duct, which is an unusual finding. e, f Axial contrast-enhanced T1-weighted VIBE images obtained in the pancreatic and late venous phase showing no enhancement of the tumor in the pancreatic phase and only minimal enhancement of the tumor in the late venous phase (arrow)
378 6.4 Malignant Tumors and Tumors with Malignant Potential
#187 Adenocarcinoma,
Ductal Changes
KEY FACTS: MRI
●Classical patterns of involvement of the main duct (Fig. 187a):
–(Apparent) occlusion (> 50% on MRCP)
–Stenosis, usually irregular with abrupt termination
–Dilation of the proximal main duct
–Double duct sign (Freeny et al. 1978; e.g., see #90, Fig. 187b–e, 188a, b); sometimes “four-segment sign” (Kim et al. 2002)
!● Side branches may be:
–Invisible (normal or obliterated)
–Dilated (obstruction; may appear like bizarre cystic pockets located adjacent to the tumor)
–Distorted/displaced
●Comments:
–Long strictures of the pancreatic duct, especially in the body or tail, are most commonly malignant (see, however,
# 164, # 167 and # 169); short strictures are more common in chronic alcoholic pancreatitis
–Projective images should be obtained routinely: subtle ductal changes may herald the presence of small tumors
References
Freeny PC, Bilbao MK, Katon RM (1976) “Blind” evaluation of endoscopic retrograde cholangiopancreatography (ERCP) in the diagnosis of pancreatic carcinoma: the “double duct” and other signs. Radiology 119 : 271–274
Kim JH, Kim MJ, Chung JJ et al. (2002) Differential diagnosis of periampullary carcinomas at MR imaging. Radiographics 22 : 1335–1352
Stewart E, Vennes J, Geenen J (1977) Atlas of endoscopic retrograde cholangiopancreatography. Mosby, St Louis, p 182
6 Pancreatic Ducts 379
a |
b |
|
c |
d |
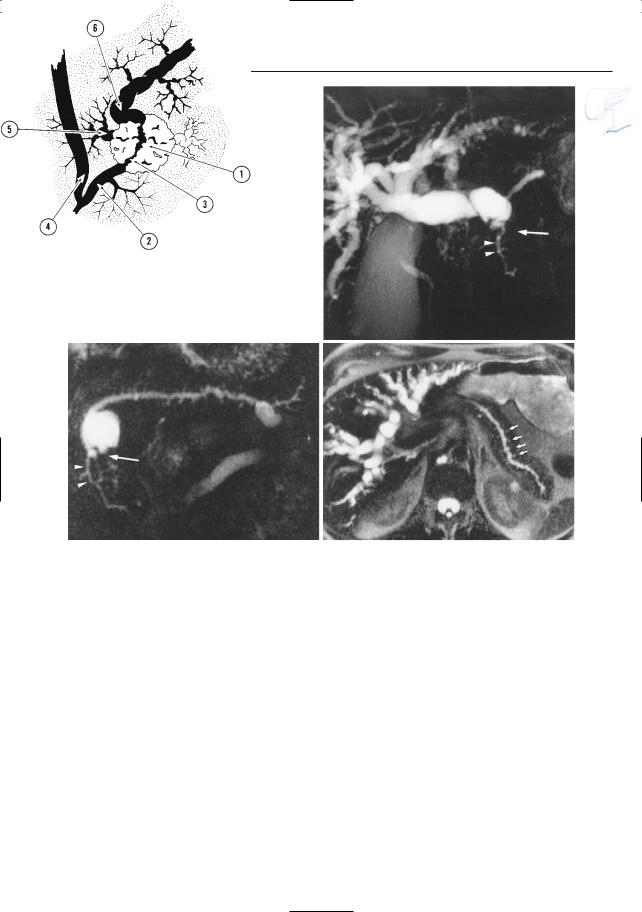
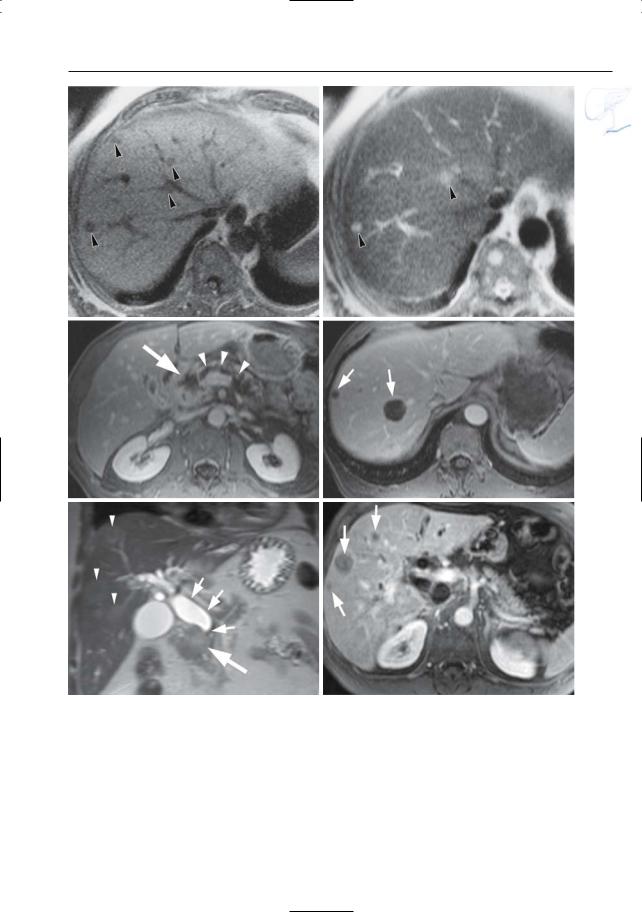
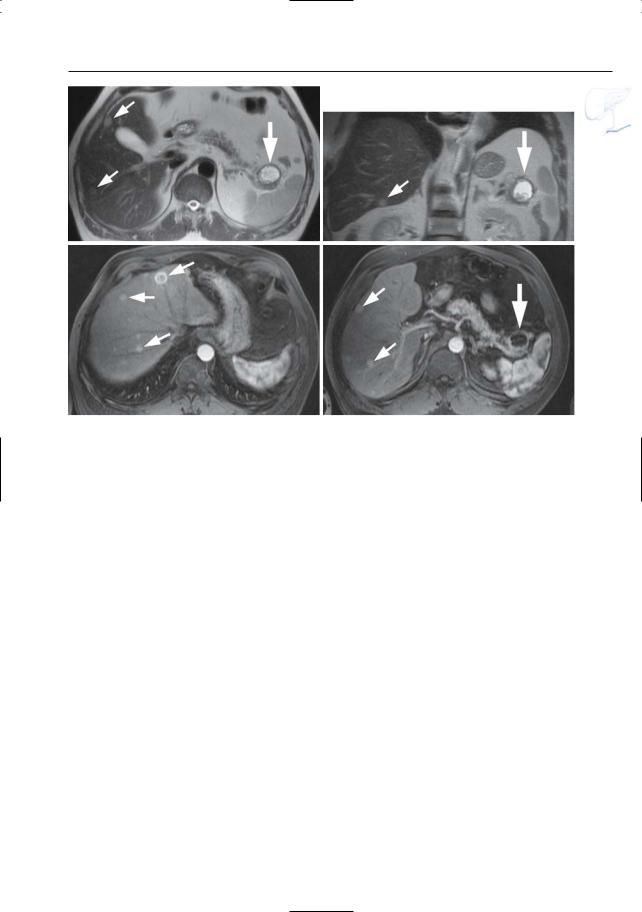
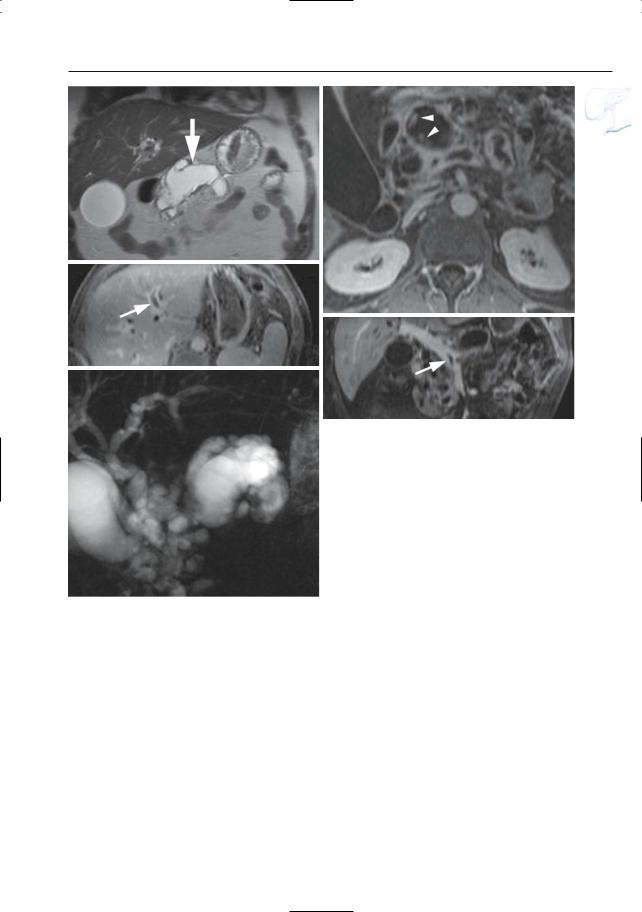
Fig. 187. a Ductal changes in pancreatic cancer. The tumor (1) causes abrupt narrowing of the pancreatic duct (2). Note the irregular contours of the stricture (3). The common bile duct (4) may be normal or stenotic at the same level.Dilated side branches are seen adjacent to the tumor mass (5). The proximal pancreatic duct shows dilation (6). Note that necrotic areas within the tumor may appear as small “cysts.” In chronic pancreatitis, dilated side branches may be seen within an inflammatory mass, rather than adjacent to the mass (see # 167). (Reprinted with permission from Stewart et al. 1997). b–d Patient with cancer of pancreatic head. Projective images showing
marked dilation of intrahepatic bile ducts with abrupt termination (arrow in b) and slightly dilated pancreatic duct that exhibits narrowing at the same level (arrow in c). Note the rather homogeneous dilation of side branches in c and the presence of a dilated side branch in the pancreatic head that is displaced by the tumor (arrowheads in b,c). The cystic lesion in the pancreatic neck proved to be a benign mucinous neoplasm (incidental finding). d Same patient. Heavily T2-weighted axial image also showing rather uniform dilation of the side branches (arrows). The final diagnosis was infiltrating adenocarcinoma of the pancreatic neck
380 6.4 Malignant Tumors and Tumors with Malignant Potential
e |
f |
g |
h |
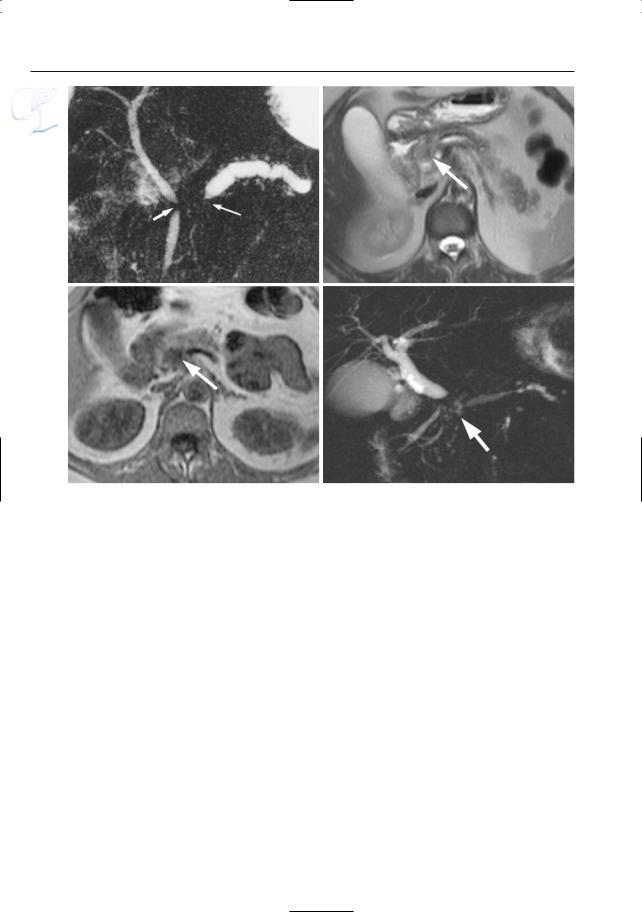
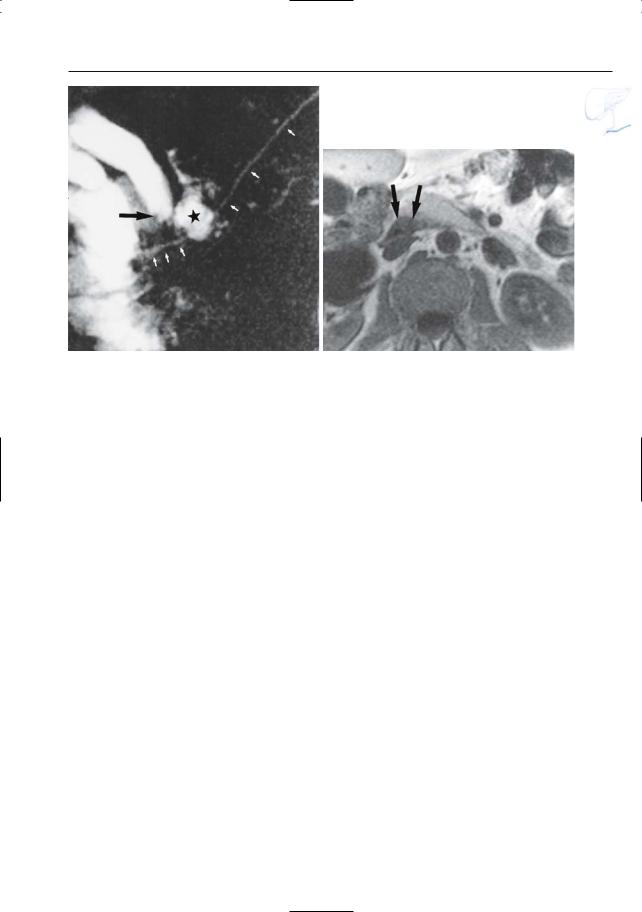
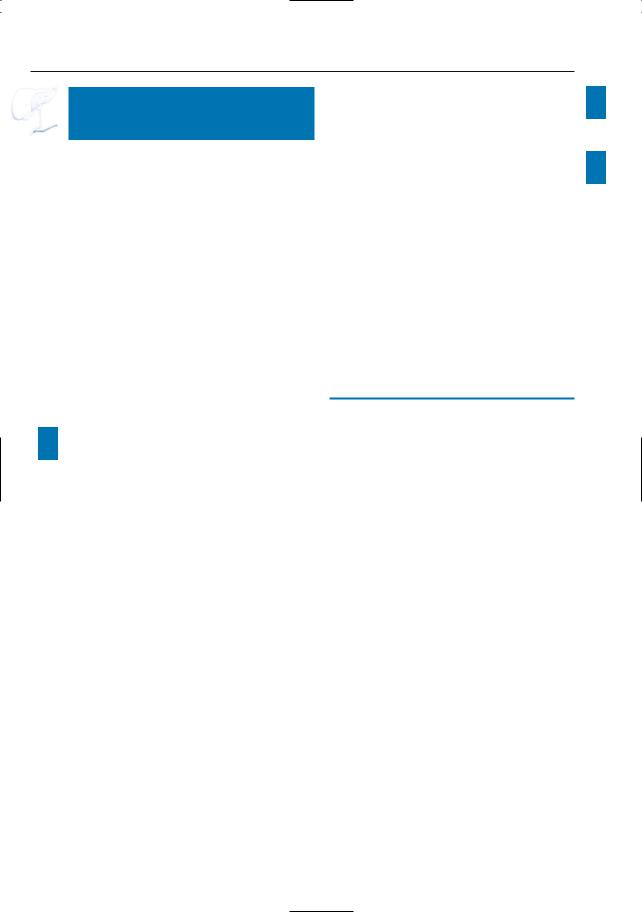
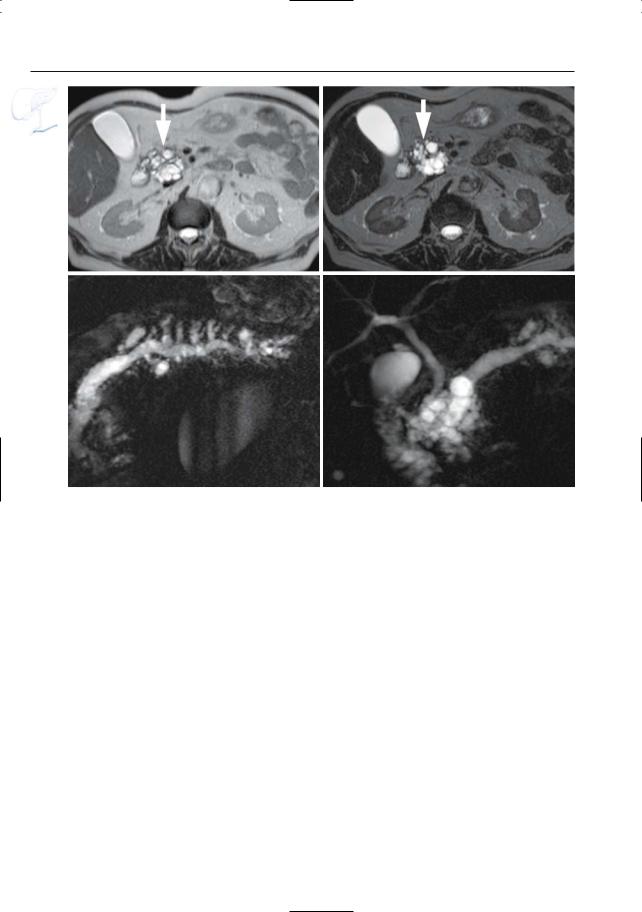
Fig. 187 a – j. (continued) e Projective image showing obliteration of the pancreatic duct associated with a short stricture of the common bile duct (double duct sign, arrows). f–h Axial T2-weighted HASTE image (f) and axial T1-weighted image (g) showing a small adenocarcinoma in the pancreatic head (arrow). As in most cases, the lesion is nearly iso-
intense to normal pancreatic parenchyma on the T2-weighted images and clearly T1-hypointense. h Projective image showing dilatation of the proximal main pancreatic and common bile duct with an abrupt obliteration of the ducts (arrow). The distal main pancreatic and common bile duct have a normal appearance (four segment sign)
6 Pancreatic Ducts 381
i |
j |
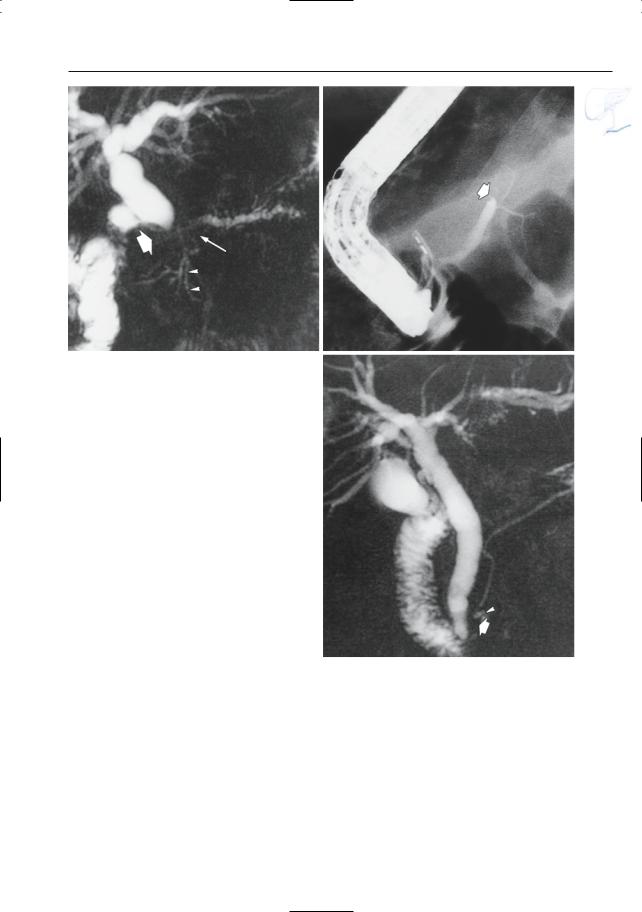
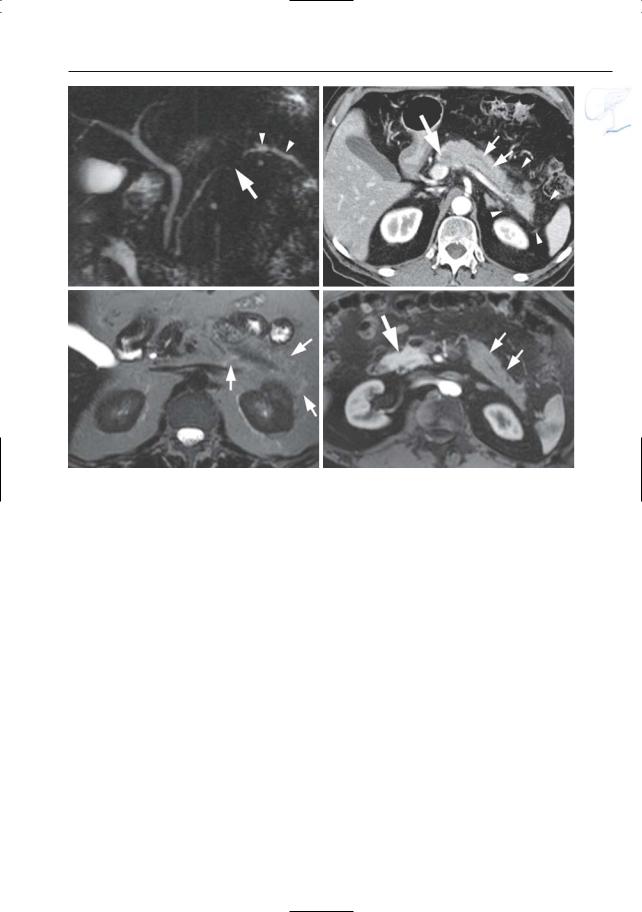
Fig. 187 a – j. (continued) i, j Axial T2-weighted HASTE image (i) showing a small adenocarcinoma in the pancreatic body (arrow) with narrowing of the main pancreatic duct and proximal dilatation
(arrow–head). j Projective image showing dilatation of the proximal main pancreatic duct (arrowheads) with irregular narrowing in the pancreatic body
(arrow)

382 6.4 Malignant Tumors and Tumors with Malignant Potential



6 Pancreatic Ducts 401
Table 197. Incidence of malignancy in neuroendocrine tumors
Tumor |
Relative frequency (%) |
Malignant (%) |
|
|
|
Insulinoma |
56 |
5–10 |
Gastrinoma |
21 |
60 |
Glucagonoma |
2.3 |
80 |
Vipoma |
1.8 |
60 |
Nonfunctioning tumors |
15 |
80–100 |
|
|
|
402 6.4 Malignant Tumors and Tumors with Malignant Potential
a |
b |
|
Fig. 197 a – c. Patient with metastatic gastrinoma. |
|
|
a T1-weighted image showing a hypointense lesion |
|
|
in the pancreatic head, corresponding to a gastri- |
|
|
noma (arrow). b Contrast-enhanced fat-suppressed |
|
|
T1-weighted image only showing the nonenhancing |
|
|
central part of the tumor (arrowhead). c Contrast- |
|
|
enhanced image obtained at a more cranial level |
|
c |
showing liver metastasis with typical rim enhance- |
|
ment (arrow) |
||
|
6 Pancreatic Ducts 407
a
b
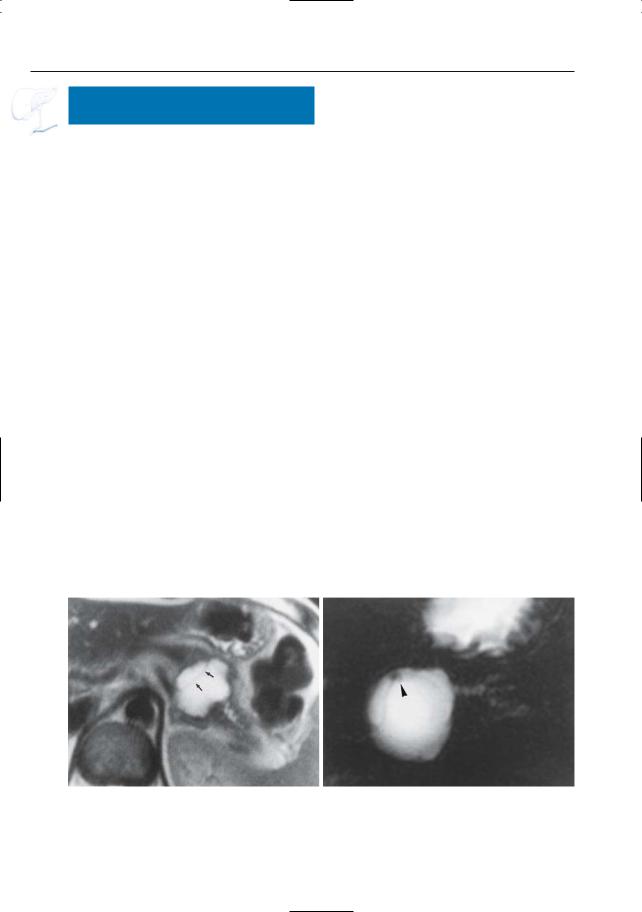
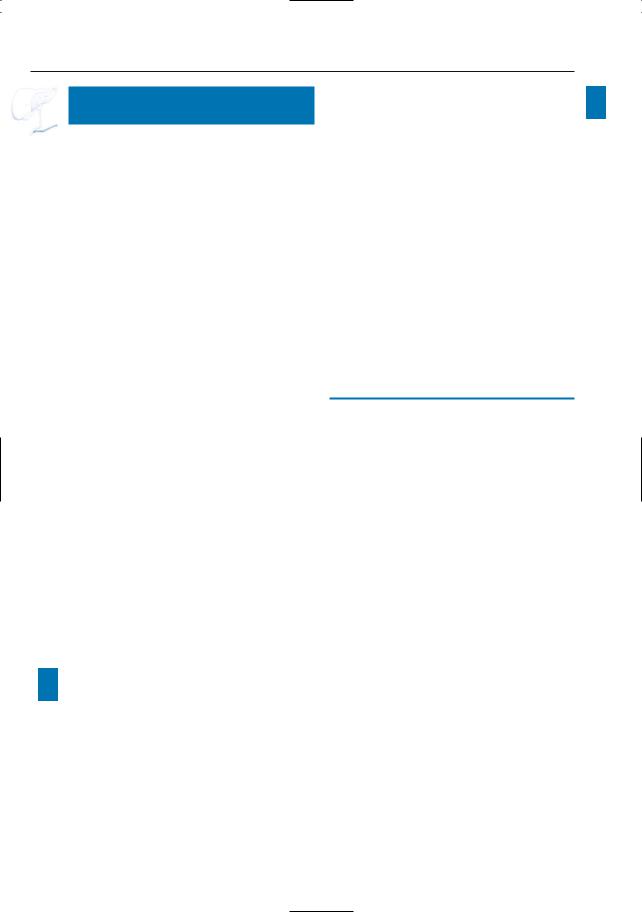
Fig. 199 a–c. a Moderately T2-weighted image showing “polycystic” mass in the uncinate process (arrows), representing a conglomerate of dilated side branches. b Projective MR image showing compression of the common bile duct. c ERCP image showing a dilated side branch containing a large filling defect (mucin plug; arrowheads). Note that the mucin plug is invisible on MRI (same intensity as fluid). Surgery was not performed in this patient because of medical contraindications.
c One year later, he presented with a large inoperable malignant mass in the pancreatic head
6 Pancreatic Ducts 409
h
i
j
k
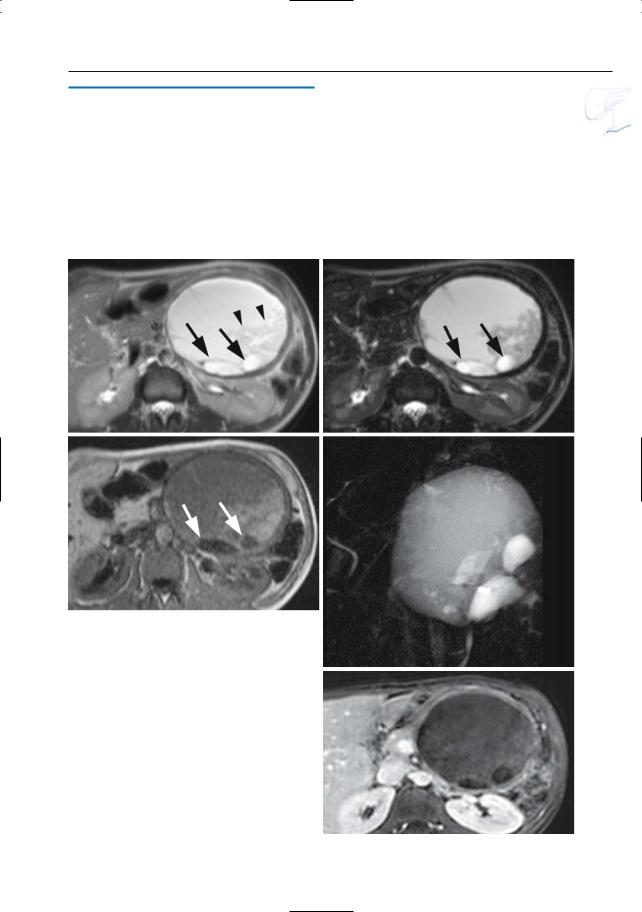
Fig. 199 h–l. Patient with a malignant IPMT of the main duct type.h Coronal T2-weighted HASTE image showing marked ductal dilatation (arrow). Axial (i, j) and coronal (k) reconstructed contrast-enhanced T1weighted VIBE images showing multiple contrast enhancing papillary protrusions in one of the larger “cystic” components due to malignant degeneration [arrowheads in (i)]. Note the presence of mucus in the main and left portal vein secondary to vascular invasion [arrows in (j, k)].l Projective image showing marked cystic pancreatic duct dilatation in the pancreatic
l head and secondary intraand extrahepatic biliary duct dilatation due to mass-effect