

Книги по МРТ КТ на английском языке / The Embryonic Human Brain An Atlas of Developmental Stages. Third Edition. 2006. By Ronan O'Rahilly
.pdf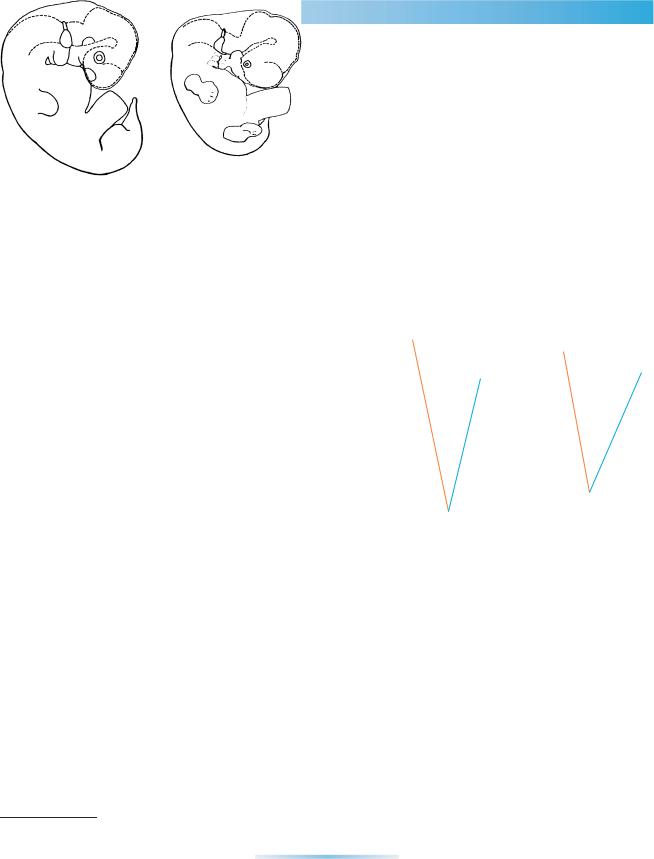
C H A P T E R 3
PRENATAL
MEASUREMENTS
Aconsiderable variety of measurements has been proposed and, as is also true of postnatal measurements, a range of values caused by variability
needs to be taken into account.
The most useful measurement in prenatal life is the greatest length (GL), taken as a caliper length without inclusion of the flexed lower limbs. The crown–rump (CR) length, which is frequently similar, is a commonly cited but unsatisfactory measurement (O’Rahilly and Muller,¨ 1984a).
In the embryonic period (the first 8 weeks), however, embryonic length (particularly when taken to one or even two decimal places) is of very little value. During that time the only reliable and indeed necessary index of developmental status is provided by morphological staging (see Chapter 4). Furthermore, it should be emphasized that the term “stage” should not be applied to a mere measurement, nor to a supposed age. Thus, the “19 mm stage” should be replaced by “at 19 mm GL”, and “the 7-week stage” by “at 7 (postfertilizational) weeks.” The greatest length is replaced after birth by the sitting height.
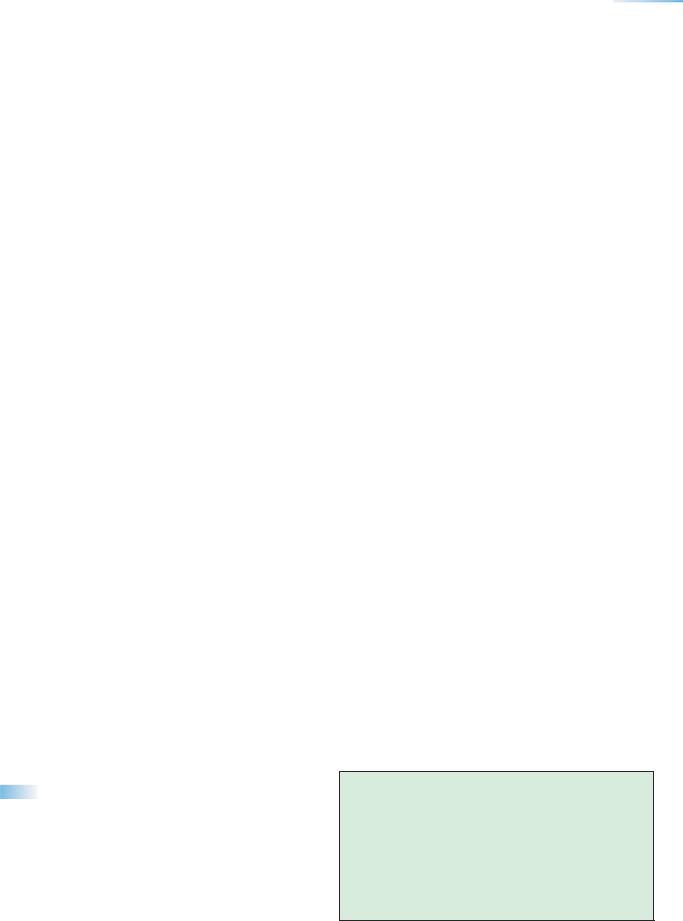
The greatest length (Fig. 3–1), as would be expected, shows variability in relation to age, and precision in estimating age can be increased by using several different measurements, as has been found in ultrasonographic studies. At 4 12 postfertilizational weeks the GL is about 5 mm, and at 8 weeks, the end of the embryonic period proper, it is approximately 30 mm.
A |
GL |
B |
GL
C
C
R
R
Figure 3–1. Outlines of embryos at (A) stage 15 and (B) stage 17 showing that the crown–rump length (CRL) and the greatest length (GL) do not necessarily coincide.
The crown–heel (CH) length includes the lower limbs and is replaced after birth by the standing height. Another useful measurement is the foot length (FL). At 8 postfertilizational weeks the CH length is about 45 mm, and the FL is approximately 4.5 mm. Additional measurements used in imaging techniques include the biparietal diameter, the head circumference, the (calcified) femoral length, and the abdominal circumference.
Where the head is defective (e.g., in anencephaly), the fetal height can be estimated from the distance between the
The Embryonic Human Brain: An Atlas of Developmental Stages, Third Edition. By O’Rahilly and Muller¨ Copyright C 2006 John Wiley & Sons, Inc.
9
10 |
C h a p t e r 3 : PRENATAL MEASUREMENTS |
spinous process of thoracic vertebra 1 and the coccyx, and from measurements of the arm, thigh, and leg (Alexandre and Pineau, 1970).
Body weight, which is about 2 to 3 g at 8 postfertilizational weeks, is variable. Later, an estimate can be obtained in vivo by special formulae based on linear measurements (e.g., biparietal diameter and abdominal circumference).
Brain weight, which is also variable, has been studied in the fetal period by a number of authors (e.g., Tanimura et al., 1971; Gilles et al., 1983), and summarizing graphs are available (Lemire et al., 1975).
Important
The most useful single prenatal measurement is the greatest length (GL) exclusive of the lower limbs.
In the embryonic period, morphological stages are much more reliable than measurements.
The GL can be determined in vivo by ultrasonography or magnetic resonance imaging; for greater precision in estimating age the GL can be combined with other measurements.
C H A P T E R 4
EMBRYONIC STAGING
Prenatal life is conveniently divided into embryonic and fetal periods. The embryonic period is that during which new features appear with great rapid-
ity, enabling subdivision to be made into morphological stages. It occupies the first 8 postfertilizational weeks. The vast majority of congenital anomalies appear during that time. The fetal period is characterized more by the elaboration of existing structures and, because of the less striking developmental changes, it has proved so far to be resistant to a morphologically based staging system.
In human embryology, staging, as distinct from mere seriation of embryos, was introduced by Mall in 1914. The system now used internationally, termed Carnegie stages by O’Rahilly, was prepared by Streeter in the 1940s. The early stages (1–9) were defined by O’Rahilly, who published them in 1973 (O’Rahilly and Muller,¨ 1987a).1 Other systems are now obsolete.
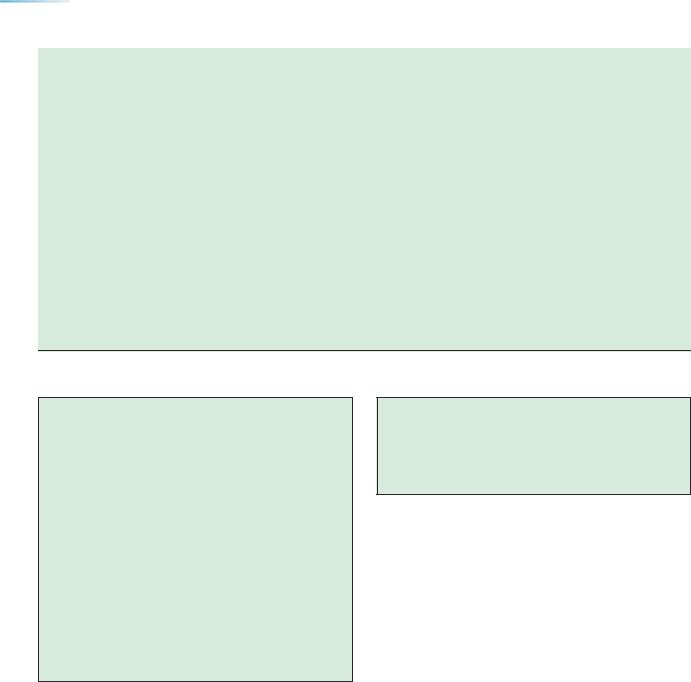
In the Carnegie system the embryonic period proper, i.e., the first 8 postfertilizational weeks of development, is subdivided into 23 stages based on external and internal morphological criteria. These stages are used throughout this book (Table 4–1).
The great advantage of morphological stages is that, in large measure, emancipation from the variables of age and measurement can be achieved for the embryonic period.
1 It is relevant to record that the late George Corner told O’Rahilly that he disliked Streeter’s term “horizon” and was pleased to see it replaced by “stage” in the 1973 monograph by O’Rahilly, who introduced the term Carnegie stage to encompass his own studies (stages 1–9) as well as those of Heuser and Corner (stage 10) and of Streeter (stages 11–23).
As information concerning ages becomes more precise, no better example can be found of the value, indeed necessity, of the morphologically based staging system, which retains its validity throughout. Moreover, comparisons are made of a number of different features (e.g., somites, neuropores, eyes, limbs), so that individual differences are rendered less significant and a certain latitude of morphological variation is taken into account.
Although external body form is of immediate access, and can even be recorded in vivo by ultrasonography, nevertheless it needs to be stressed that, particularly in certain stages (e.g., 20–22), internal morphology is an essential component of the Carnegie system. In some instances it has been found of interest to “estimate the stages” of embryos studied by ultrasound in vivo, but “exact staging by ultrasonography is not possible” (Blaas et al., 1998).
Moreover, stages should not be assigned on the basis of mere length or age, both of which are too variable. An embryo of 20 mm, for example, could almost as easily belong to stage 19 as to stage 20, because the lengths usually given for the various stages are guidelines and do not show the complete range of values. Similarly, even were an embryo known to be precisely 49 postfertilizational days in age, it could as easily belong to stage 19 as to stage 20.
In addition, the admittedly subtle but useful distinction between the embryonic and fetal periods is based on a histological criterion (the onset of marrow formation in the humerus), and neither length nor external form would be an adequate criterion.
In summary, staging is now an essential procedure in the scientific study of the human embryo, but it is necessary
The Embryonic Human Brain: An Atlas of Developmental Stages, Third Edition. By O’Rahilly and Muller¨ Copyright C 2006 John Wiley & Sons, Inc.
11
12 |
|
|
C h a p t e r 4 : EMBRYONIC STAGING |
|
|
|
|
|
|||
TABLE 4–1. Developmental Stages and Features of the Nervous System |
|
|
|||
Carnegie |
Greatest |
Approximate |
|
First appearance |
Pairs of |
stage |
length (mm) |
age (days) |
Key features of nervous system |
of neuromeres |
somites |
|
|
|
|
|
|
8 |
1 |
23 |
Neural folds and groove in stage 8b |
|
|
9 |
2 |
25 |
Mesencephalic flexure; neural groove |
P, M, Rh. A–D |
1–3 |
|
|
|
evident; otic disc |
|
|
10 |
3 |
28 |
Fusion of neural folds begins; optic |
T, D1, D2 |
4–12 |
|
|
|
primordium; otic pit |
|
|
11 |
3.5 |
29 |
Rostral neuropore closes; optic vesicles |
Rh. 1–8 |
13–20 |
|
|
|
and optic neural crest; nasal discs |
|
|
12 |
4 |
30 |
Caudal neuropore closes; secondary |
M1, M2 |
21–29 |
|
|
|
neurulation commences; |
|
|
|
|
|
adenohypophysial pouch |
|
|
13 |
5 |
32 |
Closed neural tube; retinal and lens discs |
Par., Syn., |
30–? |
|
|
|
develop; hypothalamic cell cord; medial |
Isthmus |
|
|
|
|
and lateral longitudinal fasciculi; |
|
|
|
|
|
primordium of cerebellum |
|
|
14 |
6 |
33 |
Future cerebral hemispheres; pontine |
Rostral & caudal |
|
|
|
|
flexure; torus hemisphericus & medial |
Par.; all 16 |
|
|
|
|
ventricular eminence; optic cup and lens |
neuromeres |
|
|
|
|
vesicle |
present |
|
15 |
8 |
36 |
Nasal pit; di-telencephalic sulcus; lateral |
|
|
|
|
|
ventricular eminence; hippocampal |
|
|
|
|
|
thickening; medial forebrain bundle; |
|
|
|
|
|
longitudinal zoning in diencephalon |
|
|
|
|
|
(marginal ridge) |
|
|
16 |
10 |
39 |
Olfactory tubercle; dorsal thalamus; |
|
|
|
|
|
epiphysis cerebri; neurohypophysial |
|
|
|
|
|
evagination |
|
|
17 |
13 |
41 |
Vomeronasal organ and nerve; forebrain |
|
|
|
|
|
septum; 2 to 4 amygdaloid nuclei; |
|
|
|
|
|
subthalamic nucleus; posterior |
|
|
|
|
|
commissure; red nucleus; internal and |
|
|
|
|
|
external cerebellar swellings |
|
|
18 |
15 |
44 |
Paraphysis; future corpus striatum with |
|
|
|
|
|
intrastriatal sulcus; hippocampus |
|
|
|
|
|
C-shaped; inf. & superior cerebellar |
|
|
|
|
|
peduncles; primordium of nucleus |
|
|
|
|
|
dentatus |
|
|
19 |
17 |
46 |
Olfactory bulb; nucleus accumbens; globus |
|
|
|
|
|
pallidus; choroid plexus of fourth |
|
|
|
|
|
ventricle; substantia nigra; medial |
|
|
|
|
|
accessory olivary nucleus |
|
|
20 |
20 |
49 |
Choroid plexus of lateral ventricles; septal |
|
|
|
|
|
nuclei; interpeduncular nucleus; optic |
|
|
|
|
|
fibers in chiasmatic plate |
|
|
21 |
23 |
51 |
Cortical plate in area of future insula; optic |
|
|
|
|
|
tract & lateral geniculate body |
|
|
22 |
26 |
53 |
Olfactory striae; claustrum; internal capsule; |
|
|
|
|
|
adenohypophysial stalk incomplete |
|
|
23 |
29 |
56 |
Insula indented; external capsule; caudate |
|
|
|
|
|
nucleus & putamen discernible; anterior |
|
|
commissure begins; mesencephalic Blindsacke¨; external germinal layer in cerebellum
Note: The greatest lengths and the postfertilizational ages given are approximate only. The latter have been revised to conform to current ultrasonic information.
COMPARATIVE STUDIES |
13 |
to take both external and internal morphological criteria into consideration. Neither length nor age, nor a combination of them, defines a stage in the accepted embryological meaning of the term.
At present, staging is limited to the embryonic period proper. Despite attempts to do so, no satisfactory staging system has yet been devised for the fetal period. Prenatal life, however, can conveniently be considered in terms of trimesters: (1) including the embryonic period proper (up to about 30 mm GL), and extending to some 90 or 100 mm,
(2) proceeding to about 250 mm, and (3) continuing until birth (very approximately 336 mm GL).
Staging systems are available for a number of species, two well known examples being Harrison’s staging of Ambystoma maculatus and Hamburger and Hamilton’s staging of Gallus domesticus. Such systems have arisen largely independently of each other and the numeration differs from one to another. Witschi, in the 1950s, was the major proponent of the attractive idea of a standard enumeration throughout vertebrate embryology, a suggestion that unfortunately was ignored. The Carnegie system has already been applied to a number of primate species, especially by Hendrickx and his coworkers. Unfortunately, however, most workers who study the developing mouse or rat continue to use ages instead of stages.
An ideal staging system, particularly from the viewpoint of experimental embryology, would be based entirely on external morphology. This is not always attainable, however. During some periods of development, external appearances may not change sufficiently rapidly to reflect adequately the accompanying internal changes. In the human, for example, difficulties may arise during the period from 7 to 8 postfertilizational weeks. Hence the internal structure is also important in staging. Details of internal development in staged embryos, however, seem to be incomplete or even lacking in most species other than the human. Furthermore, it should not be assumed that a given stage based on external appearances will reflect precisely similar internal features in different species. Even external features may vary among species. For example, the upper limb buds appear in the human at stage 12, whereas in the mouse they are said to begin at stage 11 and in the pig they are not distinct until stage 13; the pineal outgrowth appears in the human (and in other mammals) at stages 15–16, whereas in the chick it is said to be seen at what would correspond to stage 13.
development of the brain may parallel “equivalent stages” of the entire embryo, particularly those based on general external morphology.
Some preliminary data for equivalent stages, as distinct from equivalent ages, in the rat, mouse, and human were proposed for the early development of the brain in relation to anencephaly (Muller¨ and O’Rahilly, 1984, Tables 2 and 3). Subsequently, a general atlas of some 15 species arranged according to the Carnegie staging system appeared (Butler and Jurlink, 1987); that valuable work could serve as a point de depart´ for the construction of staged interspecies comparisons of the development of the nervous system.
“Equivalent ages” are far less desirable insofar as a major objective of staging is to escape as much as is practicable from the variables of age and linear measurements. Equivalent ages for the developing nervous system have been proposed by Clancy et al. (2001) for 95 events in 9 mammalian species, with numerous observational gaps being filled in by mathematically estimated predictions. The study suffers from the following major shortcomings, particularly with regard to the human. (1) Embryonic staging was completely ignored and replaced by “postconceptional days” that were not (for the human) based on recent ultrasonically confirmed information. (2) The human data used, admitted to be subject to “much error,” were inadequate and frequently unreliable. (3) The extensive and precise data now available for the human (Appendix 2 in the present book) were apparently unknown to the authors. (4) Comparison of the two sets of data for 37 features reveals that only 16 % are similar in timing, whereas in Table 1 of Clancy et al. (2001) 32 % are too early (by 3-16 days) and 51 % are too late (by 2-26 days), rendering their information untrustworthy.
In the fetal period, where staging is not available and where development is slower and not as clear-cut, comparisons are more difficult and are liable to be of very limited use. Incorporated in a detailed summary of the development of the nervous system of the rat (Bayer et al., 1993) are estimates in (presumably postfertilizational) weeks of what are assumed to be corresponding features in the human. The “assumptions,” “approximations,” and “extrapolations” involved in such studies inevitably lead to numerous pitfalls. (The inadequate account of the embryonic period in the above mentioned article had already been superseded by the works cited here in Table 23-2).
COMPARATIVE STUDIES
A valuable investigation of the brain of the rhesus monkey was undertaken by Gribnau and Geijberts, and efforts have been made to compare the development of the brain in various mammals (e.g., by Ashwell et al., 1996), but a comparative study similar in detail to the present work on the human awaits the future. Such investigations are needed in order to assess to what extent “equivalent stages” in the
Important
Morphological staging is essential for precise embryological studies.
In the embryonic period, external and internal criteria are used in the assignment of 23 internationally accepted morphological stages.
In the fetal period, a satisfactory system of morphological staging is not at present available.

C H A P T E R 5
PRENATAL AGE
Prenatal age extends from fertilization to birth and hence should be given as postfertilizational weeks (or days). Ovulation is close to the time of
fertilization (which, incidentally, is not a moment), so that postovulatory weeks or days (i.e., the time since the last ovulation) are an acceptable indication of age.
“Gestation” merely means pregnancy (“being with child”) and lacks any technical precision, so that “gestational age” and “gestational weeks or days” are completely ambiguous, scientifically useless, and should be abolished (O’Rahilly an Muller,¨ 2000). In obstetrics, menstrual weeks are generally and conveniently used and are assumed to be approximately a fortnight greater than the (postfertilizational) age. The use of the LMP measures the period of amenorrhea, when for the first two weeks no embryo existed (!), so that menstrual weeks are not age. Hence the designation menstrual “age” should not be used. In other words, an 8-week embryo may be assigned 10 menstrual weeks, but not said to have a menstrual “age” of 10 weeks.
In the embryonic period, once the stage of an embryo is known, its presumed postfertilizational age can be assessed from an appropriate table or graph (O’Rahilly and Muller,¨ 1987a), such as Table 4–1. It is likely, however, that variation may be greater than previously thought, and some of the ages accepted for early embryos may perhaps be slightly
too low. According to studies with transvaginal sonography (Dr. Josef Wisser, personal communication, 1992), embryos of stages 6 to 16 may commonly have ages 1 to 3 (more usually 3 to 5) days more than the previous embryological norms.
It has already been pointed out that, in embryological usage, (1) external body form and (2) internal morphological status are the criteria for staging, and (3) greatest embryonic length, although it is not a determining factor, is not entirely neglected. A further characteristic, (4) postfertilizational age, is rarely available and generally has to be estimated from the other three parameters.
Considerable progress in imaging (e.g., by the use of transvaginal sonography) has enabled an estimate, but only an estimate, of the stage of a given embryo to be made in vivo. This is based on parameters 1 and 3 mentioned above, and No. 4 is sometimes also known. No. 2, internal morphological status, however, is not adequately identifiable, at least at the histological level, and hence precise staging remains an embryological rather than a clinical procedure. This distinction is particularly important in very early and in very late embryonic stages.
The ages at which the chief features of the brain can be detected in present usage in vivo by ultrasound during the first trimester are listed in Table 5–1.
The Embryonic Human Brain: An Atlas of Developmental Stages, Third Edition. By O’Rahilly and Muller¨ Copyright C 2006 John Wiley & Sons, Inc.
15
16 |
|
C h a p t e r 5 : PRENATAL AGE |
|
||
TABLE 5–1. Chief Features of the Brain Found by Ultrasound During Trimester 1a |
||
Postfertilizational |
|
|
Weeks (Age) |
Postmenstrual Weeks |
Features |
|
|
|
5 |
7 |
First indication of brain |
5–6 |
7–8 |
Cerebral hemispheres, lateral ventricles, wide interventricular foramina |
|
|
Future third ventricle |
|
|
Mesencephalon and future aqueduct |
|
|
Rhombencephalon and fourth ventricle |
6–7 |
8–9 |
Choroid plexuses of lateral ventricle |
|
|
Telencephalon, diencephalon, mesencephalon, metencephalon, myelencephalon |
|
|
Cerebellum, pontine flexure, lateral recesses of fourth ventricle |
7–8 |
9–10 |
Falx cerebri |
|
|
C-shaped lateral ventricles |
|
|
Narrower third ventricle |
|
|
Isthmus prosencephali (between third ventricle and aqueduct) |
8–10 |
10–12 |
Growing thalami |
|
|
Cerebellar hemispheres seem to meet |
|
|
Cerebellar peduncles |
Tentorium cerebelli
Fourth ventricle divided by choroid plexus
a Based on data in Blaas (1999) and Timor-Tritsch et al. (2001).
Important
Prenatal age is postfertilizational by definition, although an acceptable alternative is postovulatory.
In the embryonic period, age is assessed from the standard morphological stage of the embryo.
When the embryonic length (GL) is within the range 3–30 mm, a very good estimate of age can be obtained by adding 27 to the length.
In the fetal period, age is estimated from measurements such as the greatest length (GL) taken in vivo by ultrasonography or magnetic resonance imaging. In obstetrics a useful preliminary criterion, although it is not age, is the postmenstrual interval. The term “menstrual age” is incorrect and the scientifically useless qualification “gestational” should not be used.
Concluding Note
It is recommended that decreasing confidence be given to the number of days assigned to an individual embryo or fetus, and that increasing precedence be awarded to weeks and half-weeks.

C H A P T E R 6
TERMINOLOGY
The nomenclature used in this book is mostly that which is accepted internationally and is in current anatomical usage. Examples of terms not employed,
including some comparative terms that are inappropriate to the human (e.g., branchial instead of pharyngeal) are given in Table 6–1.
Eponyms are by no means always justifiable historically; they convey no morphological information, they add unnecessary complications, and hence are to be avoided wherever possible. The island of Reil, for example, is much more simply rendered as merely the insula. Similarly, the fissures of Rolando and Sylvius, which are actually sulci (!), are much better given as the central and lateral sulci, respectively.
In early development, such terms as anterior and posterior should be avoided. Appropriate terms for the embryo include rostral and caudal, dorsal and ventral. As in adult anatomy, the unofficial and unnecessary terms midsagittal, for median, and parasagittal, for merely sagittal, should not be used. Sagittal planes, including the median plane, are used as in adult anatomy. Transverse and coronal planes, however, generally refer to the trunk prenatally and are frequently unclear when applied to the flexed head, as found in the embryo (Fig. 6–1).
Three main planes are used in anatomy: horizontal and two vertical planes, coronal and sagittal. One of the sagittal planes is median. One of the horizontal planes, the orbitomeatal, is used to ensure that the head is in the anatomical position. Strictly coronal planes are vertical planes that are at a right angle to both the orbitomeatal and the median plane. Prenatally, however, the situation is complicated by the curvature of the body and the flexion of the head. Consequently, a transverse section of the trunk (a horizontal section in the adult) is not parallel to the orbitomeatal plane (Fig. 6–1). Similarly, a coronal section of the prenatal trunk does not correspond to a coronal section of the adult head. These considerations, which are important in prenatal imaging, need to be kept in mind, even though a satisfactory resolution of the problem has yet to be achieved. When an unspecific plane is encountered in ultrasonic studies, the term “anyplane” is sometimes used.
The terms used for the divisions and main subdivisions of the brain, as provided by Wilhelm His in preparation for the Basel Nomina anatomica of 1895 are summarized in Table 6–2 and Figure 6–2. The terms are basically those given by von Baer, with the addition of the isthmus rhombencephali.
A Glossary of terms relating to human neuroembryology is provided later in the book.
The Embryonic Human Brain: An Atlas of Developmental Stages, Third Edition. By O’Rahilly and Muller¨ Copyright C 2006 John Wiley & Sons, Inc.
17