

Книги по МРТ КТ на английском языке / MRI for Orthopaedic Surgeons Khanna ed 2010
.pdf20 |
I Initial Concepts |
|
|
|
|
|
|
Humeral head |
Glenoid |
Acromion |
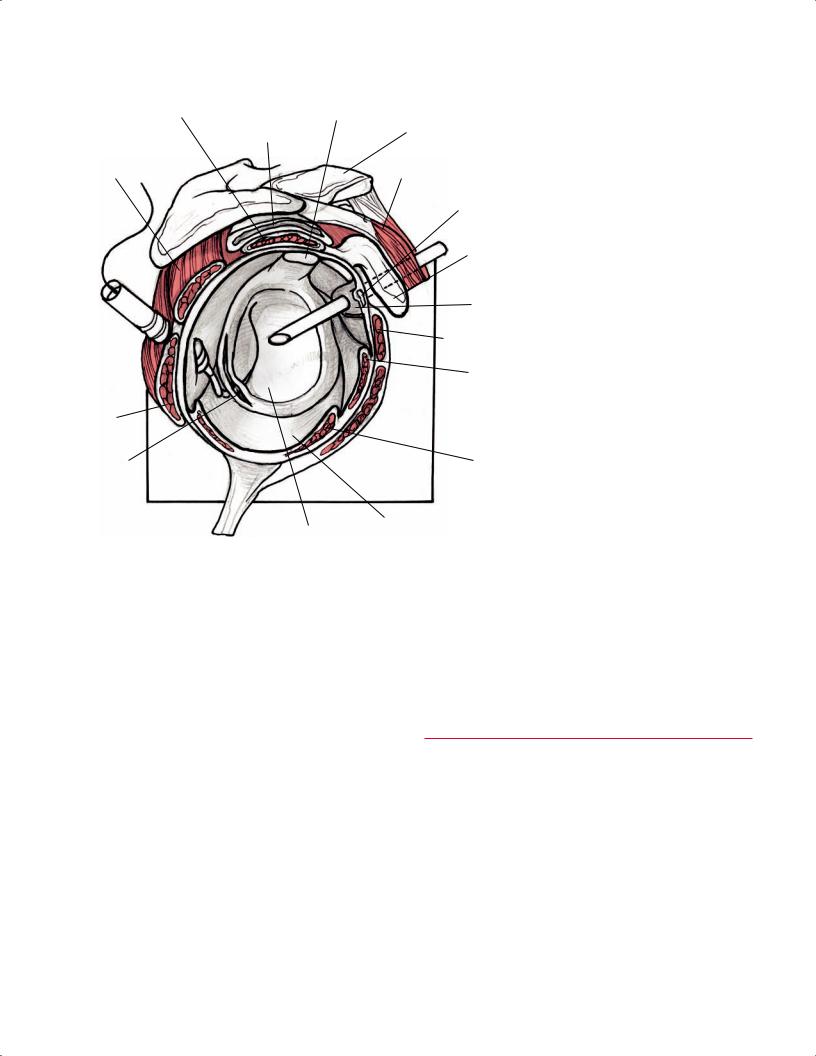
Fig. 2.5 A coronal illustration of the right shoulder at the |
|
|
cartilage |
|
|
|
|
Subacromial |
labrum superior process |
level of the supraspinatus muscle and tendon showing the |
||
|
|
||||
|
bursa |
|
|
|
glenoid and humeral head cartilage and the superior and |
|
|
|
|
|
|
|
Deltoid m. |
|
|
|
inferior glenoid labrum. |
|
Supraspinatus m. |
Conjoined |
|
tendon |
Scapula |
|
|
Humeral |
Articular |
head |
|
|
surface of |
|
glenoid |
Deltoid m. |
Subscapularis m. |
|
Axillary n. |
IGHL |
Teres |
Axillary pouch |
|
|
major m. |
|
Posterior humeral |
|
||
|
|
||
circumflex a. |
|
|
|
images. The superior and inferior glenoid labrum are seen as low signal intensity structures, in contrast to high signal intensity fluid on T2-weighted images. The axillary pouch usually is collapsed or has a small amount of fluid in the recess (Fig. 2.5). Humeral head articular cartilage, intermediate in signal intensity on T1-weighted and T2-weighted images, is
Trapezoid lig.
AC lig.
Conoid lig.
Acromion |
Clavicle |
interposed between the low signal intensity supraspinatus tendon superiorly and the cortex inferiorly.
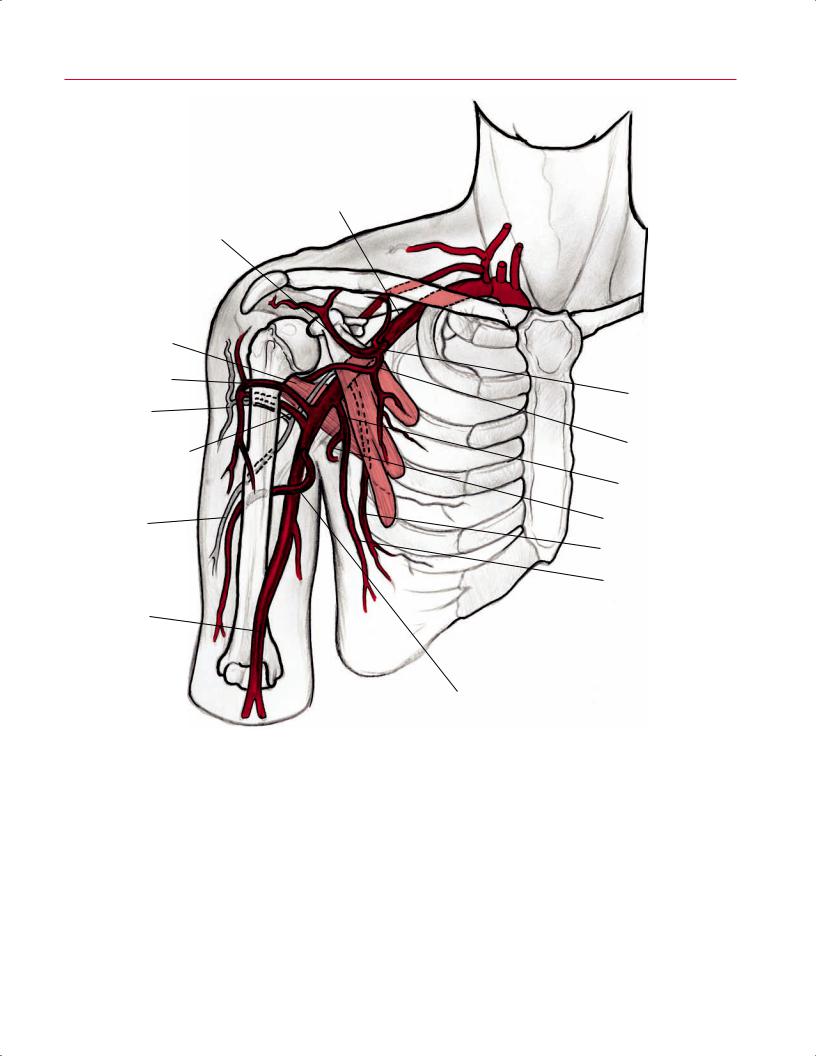
The subclavian artery courses laterally between the anterior scalene and middle scalene muscles. The axillary artery continues from the subclavian artery at the lateral border of the first rib. Branches of the axillary artery are the supreme thoracic artery, thoracoacromial artery, lateral thoracic artery, subscapular artery, and anterior and posterior humeral circumflex arteries. The brachial artery continues from the axillary artery at the lateral border of the teres major muscle (Fig. 2.7). The brachial artery passes posterior to the bicipital aponeurosis, and its branches provide arterial flow to the forearm and hand.
Coracoacromial lig.
Greater |
|
|
tuberosity |
|
|
Groove for |
Pectoralis minor tendon |
|
deltoid tendon |
||
|
||
Lesser tuberosity |
|
|
|
Coracobrachialis tendon |
|
|
Short head of biceps tendon |
Fig. 2.6 A 3D coronal illustration of the right shoulder, identifying the insertion locations of the rotator cu tendons at the greater and lesser tuberosities of the humerus. Also shown are the coracoclavicular and coracoacromial ligaments and other ligaments that stabilize the shoulder.
Sagittal Oblique Images
Sagittal oblique images, obtained in a plane that is perpendicular to the supraspinatus tendon, should extend from the most lateral aspect of the humeral head to the midscapula (to evaluate rotator cu muscle atrophy). The osseous structures (Fig. 2.3B) can be used to orient oneself to the location of the rotator cu muscles, tendons, and other nonosseous structures (Fig. 2.8). These oblique images are well suited for evaluating the rotator cu muscles and tendons (Fig. 2.9), coracoacromial arch, rotator interval, and acromial morphology.3 The glenoid labrum and the long head of the biceps can also be evaluated on the sagittal oblique images. However, both structures are better visualized on axial and coronal oblique images. Sagittal oblique images should be
2 Normal MRI Anatomy of the Musculoskeletal System 21
Subclavian a.
Acromial br. of thoracoacromial a.
Subscapularis m.
Anterior humeral circumflex a.
Axillary n.
Posterior humeral circumflex a.
Radial n.
Brachial a.
Thoracoacromial trunk
Pectoral br.
Subscapular a.
Circumflex scapular a.
Lateral thoracic a.
Thoracodorsal a.
Deep brachial a.
Fig. 2.7 A 3D coronal illustration of the neurovascular structures of the right shoulder and arm showing the subclavian, axillary, and brachial arteries, as well as smaller branch vessels such as the anterior
humeral circumflex artery, a tributary of the axillary artery, which is seen coursing anterior to the surgical neck of the humerus.
22 |
I Initial Concepts |
|
|
|
Supraspinatus m. |
Long head of |
Fig. 2.8 A 3D sagittal illustration of the right |
|
biceps tendon |
glenoid showing a labral tear. |
|
|
|
||
|
|
Subacromial |
Clavicle |
|
|
bursa |
|
|
Infraspinatus m. |
|
Deltoid m. |
|
|
|
Superior glenohumeral lig. |
|
|
|
Coracoid |
|
|
|
process |
|
|
|
Rotator |
|
|
|
interval |
|
|
|
Subscapularis m. |
|
|
|
MGHL |
|
Teres |
|
|
|
minor m. |
|
|
|
Glenoid |
|
IGHL |
|
labral tear |
|
|
Inferior
joint capsule
Glenoid fossa
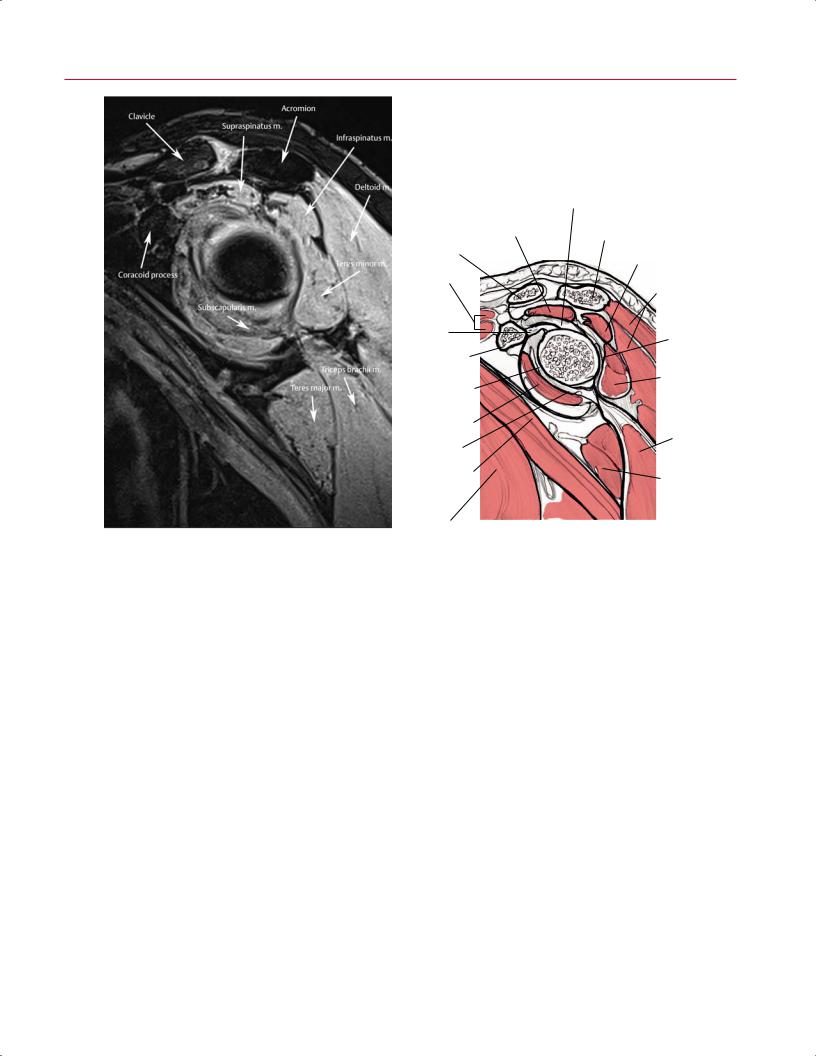
reviewed systematically from medial to lateral. Medial sagittal sections display the clavicle and AC joint in profile. On midsagittal and lateral sagittal images, the supraspinatus, the infraspinatus, and the confluence of the cu tendons are visualized between the acromion and the superior articular surface of the humeral head. The supraspinatus originates from the supraspinatus fossa of the scapula, and the infraspinatus originates from the infraspinatus fossa of the scapula. The teres minor originates from the posterolateral aspect of the scapula. All three of these rotator cu structures (the supraspinatus, infraspinatus, and teres minor) insert at the greater tuberosity of the humerus: the supraspinatus, along the most superior aspect of the greater tuberosity; the infraspinatus, along the middle facet of the greater tuberosity; and the teres minor, along the inferior facet of the greater tuberosity. The subscapularis is the most anterior rotator cu muscle, and it originates from the subscapularis fossa of the scapula. It is unique in that it is the only rotator cu structure to insert along the lesser tuberosity of the humerus rather than the greater tuberosity (Fig. 2.6). The biceps tendon can be followed from medial to lateral as it courses from its in-
traarticular origin within the synovial sheath to its more lateral extracapsular location in the bicipital groove. The long head of the biceps originates from the supraglenoid tubercle, and the short head of the biceps originates from the coracoid (Fig. 2.3).
■ Elbow
Axial Images
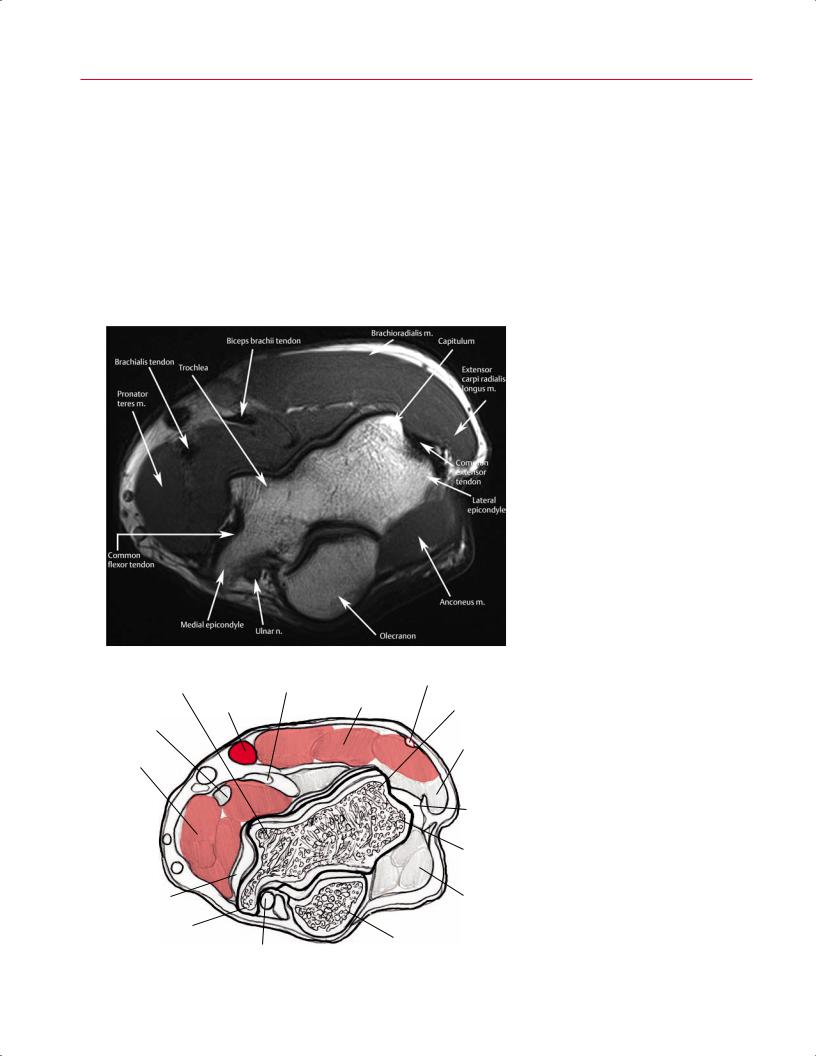
Axial images of the elbow should extend from above the humeral epicondyles (Fig. 2.10) to a level distal to the radial tuberosity. The tendons related to the elbow are best evaluated in the axial plane. The major muscles in the anterior compartment of the arm are the biceps brachii and the brachialis; the major muscle in the posterior compartment is the triceps brachii. Ventrally, the biceps tendon is seen as a low signal intensity structure, which courses from its musculotendinous junction, beneath the lacertus fibrosis, to its insertion on the radial tuberosity (Fig. 2.11). Some fibers of
2 Normal MRI Anatomy of the Musculoskeletal System 23
|
|
Biceps labral complex |
||
|
|
Supraspinatus m. |
Acromion |
|
|
|
|
||
|
Clavicle |
|
Infraspinatus m. |
|
|
|
|
||
|
Deltoid m. |
|
Deltoid m. |
|
|
|
|
(posterior) |
|
|
Coracohumeral |
|
Posterior |
|
|
lig. |
|
labrum |
|
|
Coracoid |
|
|
|
|
process |
|
Teres |
|
|
|
|
||
|
Middle & superior |
|
minor m. |
|
|
glenohumeral ligs. |
|
|
|
|
(conjoined) |
|
|
|
|
Subscapularis m. |
|
Triceps |
|
|
|
|
brachii m. |
|
|
Anterior IGHL |
|
|
|
|
Coracobrachialis |
|
Teres |
|
|
m. |
|
||
|
|
major m. |
||
|
|
|
||
|
Pectoralis |
|
|
|
A |
|
|
B |
|
major m. |
|
|
||
Fig. 2.9 A sagittal proton-density image with fat suppression (A) and artist’s sketch (B) of the left shoulder at the level of the rotator cu muscles. Although it takes some practice to evaluate the shoulder in
the distal biceps brachii also contribute to the bicipital aponeurosis. The aponeurosis extends from the myotendinous junction of the biceps to the fascia overlying the anteromedial muscles (flexors and pronators) and is identified as a thin, black, low signal intensity line on an axial image. The biceps brachii spans the shoulder and elbow joints and has a short and long head. The brachialis originates from the anterior aspect of the distal humerus, and its tendon courses immediately deep and slightly medial to the biceps and inserts on the ventral surface of the coronoid process of the ulna. The brachialis muscle is intermediate in signal intensity. Posteriorly, the triceps brachii has three heads with three separate origins; the distal triceps tendon attaches to the olecranon process of the ulna (Figs. 2.12 and 2.13).
Axial images also show the muscle architecture well. Because of the relative complexity of the forearm musculature compared with the arm musculature, forearm muscles are often grouped by location (superficial or deep) or by compartment (anterior, lateral, or posterior). Both classification
the sagittal plane, the rotator cu muscles are often best visualized on this view.
schemes are acceptable, although individual radiologists or clinicians may have a preference; it may be helpful to review both classification schemes.
Muscle Classification by Location
There are seven superficial muscles within the dorsal aspect of the proximal forearm:
•Extensor carpi radialis brevis
•Extensor carpi radialis longus
•Brachioradialis
•Extensor digitorum
•Extensor digiti minimi
•ECU
•Anconeus (not always present)
Five superficial muscles are found within the volar aspect of the proximal forearm:
24 I Initial Concepts
• Pronator teres |
dus (for the superficial and deep muscles within the distal |
|
• Flexor carpi radialis |
forearm, see Wrist, below). |
|
• Flexor carpi ulnaris |
|
|
• Flexor digitorum superficialis |
Muscle Classification by Compartment |
|
• Palmaris longus (absent in approximately 15% of the |
||
|
||
population7) |
The anterior compartment of the forearm contains the fol- |
|
In the proximal forearm, there is only one superficial |
lowing five muscles: |
|
|
||
muscle within the dorsal aspect, the supinator, and one deep |
• Pronator teres |
|
muscle within the volar aspect, the flexor digitorum profun- |
• Flexor carpi radialis |
A
Trochlea |
Biceps brachii tendon |
Cephalic v. |
|
|
|
||
|
|
|
|
|
|
Brachioradialis m. |
Capitulum |
Brachial a.
Brachialis tendon
Extensor carpi radialis longus m.
Pronator teres m.
|
|
Common |
|
|
extensor |
|
|
tendon |
|
|
Lateral |
|
|
epicondyle |
|
Common flexor |
Anconeus m. |
|
tendon |
|
|
|
|
|
Medial epicondyle |
Olecranon |
B |
|
|
|
Ulnar n. |
|
|
|
Fig. 2.10 An axial proton-density image (A) and artist’s sketch (B) of the left elbow at the level of the humeral epicondyles illustrating the muscle architecture of the distal arm. The biceps brachii tendon, the common flexor tendon, and the common extensor tendon show normal thickness and low signal intensity.
|
|
|
|
2 Normal MRI Anatomy of the Musculoskeletal System |
25 |
|||
|
|
• Flexor digitorum superficialis |
• Extensor carpi radialis brevis |
|
|
|
|
|
|
|
• Flexor carpi ulnaris |
|
• Extensor digitorum |
|
|
|
|
|
|
• Flexor digitorum profundus |
Two muscles are found in the posterior compartment of the |
|
||||
|
|
|
|
|
||||
|
There are four muscles in the lateral compartment of the forearm: |
|
|
|
|
|||
|
forearm: |
|
• Anconeus |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
• Brachioradialis |
|
• ECU |
|
|
|
|
|
|
• Extensor carpi radialis longus |
|
|
|
|
|
|
|
|
Articular capsule |
Anterior band of UCL |
|
|
|
|
|
|
|
|
|
|
|
|
||
|
|
|
|
Humerus |
|
|
|
|
|
|
Biceps brachii tendon |
|
|
|
|
|
|
|
|
|
|
Triceps brachii |
|
|
|
|
|
|
|
|
tendon |
|
|
|
|
|
|
|
|
|
Articular capsule |
|
||
|
|
|
|
Posterior |
|
|
|
|
|
|
|
|
bundle |
|
|
|
|
|
|
|
|
|
Medial |
|
||
|
|
|
|
|
epicondyle |
|
||
|
|
|
|
Lateral |
|
|
|
|
|
|
|
|
epicondyle |
UCL |
|
||
|
|
|
|
|
|
|||
|
|
Oblique cord |
Transverse lig. |
|
|
|
|
|
|
|
Tubercle on coronoid process |
RCL |
|
|
|
|
|
|
|
|
|
Annular lig. |
|
|
|
|
|
|
|
|
Oblique |
Brachialis m. insertion |
|
||
|
|
|
|
cord |
|
|||
|
|
|
|
|
|
|
|
|
|
|
|
|
Radius |
Ulna |
|
||
|
|
|
|
|
|
|
|
|
A |
|
|
|
B |
|
|||
|
|
|
|
|
||||
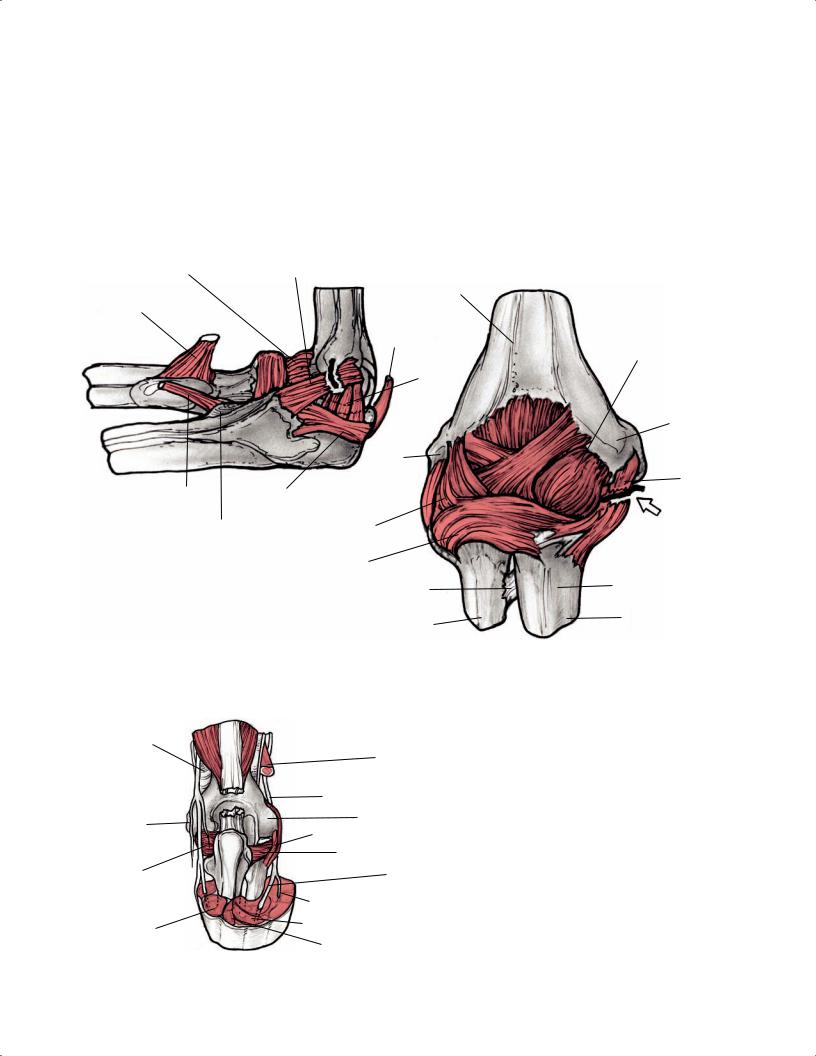
Fig. 2.11 Lateral (ulnar side) (A) and posterior (B) 3D illustrations of the left elbow showing the ligamentous structures that stabilize the elbow joint and a tear of the UCL (arrow on B).
Medial intermuscular septum
Ulnar n. 
Medial epicondyle
UCL
Flexor carpi ulnaris m.
Lateral intermuscular  septum
septum
Brachioradialis tendon
 Triceps tendon
Triceps tendon
Radial n.
Lateral epicondoyle
RCL
Annular lig.
Posterior interosseous n.
Superficial br. of radial n.
ECU m.
Anconeus m.
Fig. 2.12 A posterior 3D illustration of the right elbow showing the insertion of the triceps tendon (cut) onto the olecranon process of the ulna. Also seen are other neural and ligamentous structures.
26 |
I Initial Concepts |
|
|
|
|
Biceps m. |
Brachialis m. |
Triceps m. |
Fig. 2.13 A sagittal illustration of the elbow at the ulnotroch- |
lear articulation showing an avulsion of the distal triceps tendon near its insertion.
Triceps tendon avulsion
Olecranon
Trochlea
Trochlear
 ridge
ridge
Olecranon Biceps  bursa
bursa
tendon 
 Ulna
Ulna
Flexor digitorum profundus m.
Brachioradialis m. |
Flexor digitorum superficialis m. |
|
|
Pronator teres m. |
|
Brachialis m.
Biceps tendon
Biceps m.
Brachial a.
Median n.
Cephalic v.
Brachioradialis m.
Radial n.
Extensor carpi radialis longus m.
Extensor carpi radialis brevis m.
Capitellum |
|
|
Lateral epicondyle |
|
|
Level of |
|
|
cross-section |
Anconeus m. |
Olecranon |
|
||
|
|
Pronator teres m.
Trochlea
Medial epicondyle
Ulnar n.
Cubital tunnel retinaculum
Common flexor tendon
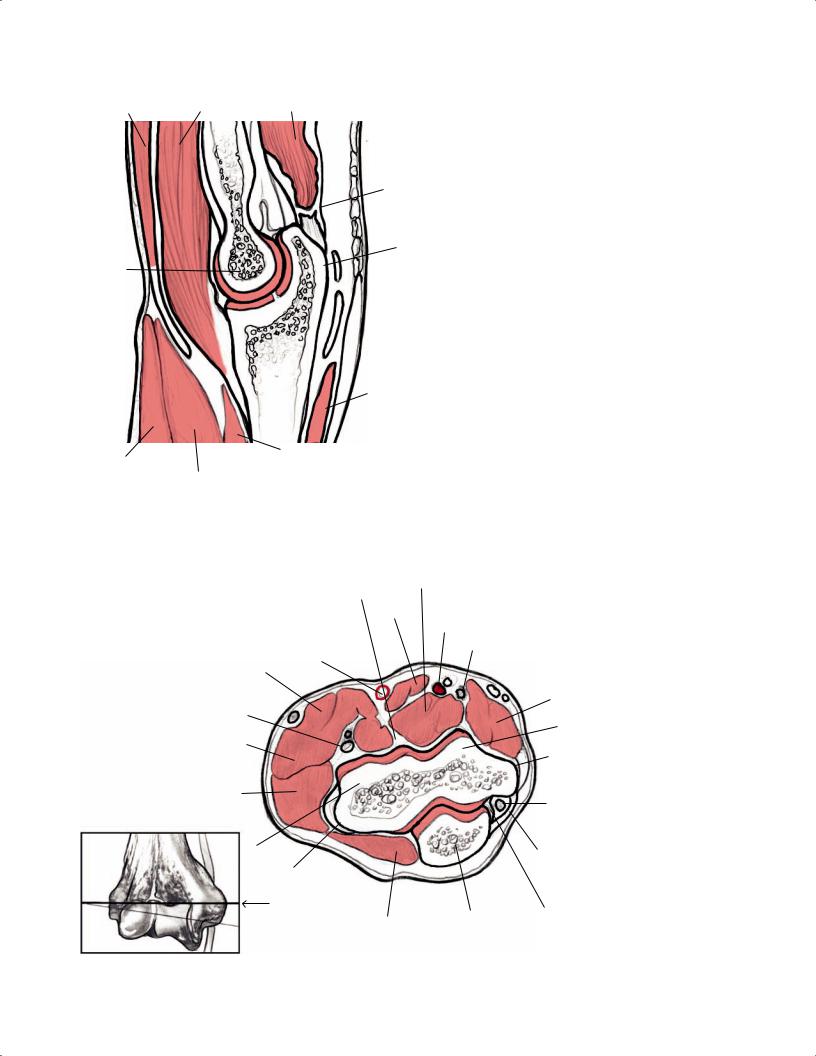
Fig. 2.14 An axial illustration of the elbow at the level of the medial and lateral epicondyles (see inset) showing the radial and ulnar nerves and the common flexor and common extensor tendons.
|
|
2 Normal MRI Anatomy of the Musculoskeletal System 27 |
||
|
|
|
|
|
|
Brachial a. |
Not surprisingly, given their shared origin at the medial epi- |
||
|
Median n. |
condyle via the common flexor tendon, the pronator teres |
||
Radial |
and flexor carpi radialis are both involved in medial epicon- |
|||
|
||||
collateral a. |
|
dylitis. |
||
|
|
|||
|
|
The medial epicondyle is not only the origin of the com- |
||
|
Ulnar n. |
mon flexor tendon, but also the origin of the MCL (or UCL). |
||
Radial n. |
The common flexor tendon is superficial to the MCL, which |
|||
|
||||
|
also attaches to the sublime tubercle, the most proximal and |
|||
|
|
|||
|
Superior |
medial portion of the ulna. The sublime tubercle is a help- |
||
Middle |
ulnar |
ful landmark, which can be used to easily identify the MCL, |
||
collateral a. |
||||
collateral a. |
|
especially given that the common flexor tendon and the MCL |
||
|
|
are similarly low in signal intensity. |
||
Superficial radial n. |
|
The LUCL and RCL are low signal intensity structures orig- |
||
|
inating along the lateral epicondyle in the lateral compart- |
|||
|
|
|||
|
|
ment of the elbow (Fig. 2.11). The common extensor tendon |
||
|
Medial |
is located more posteriorly but also attaches to the lateral |
||
|
epicondyle |
epicondyle (Fig. 2.14). It is seen in cross-section on axial |
||
|
|
|||
Anterior |
Median n. |
images and is low in signal intensity. The common extensor |
||
interosseous n. |
(continued ) |
tendon is shared by several extensor muscles in the forearm, |
||
|
||||
|
Anterior ulnar |
including the following: |
||
|
collateral a. |
|
|
|
Posterior ulnar collateral a.
Common interosseous a.
Ulnar a.
Radial a. |
Posterior interosseous a. |
|
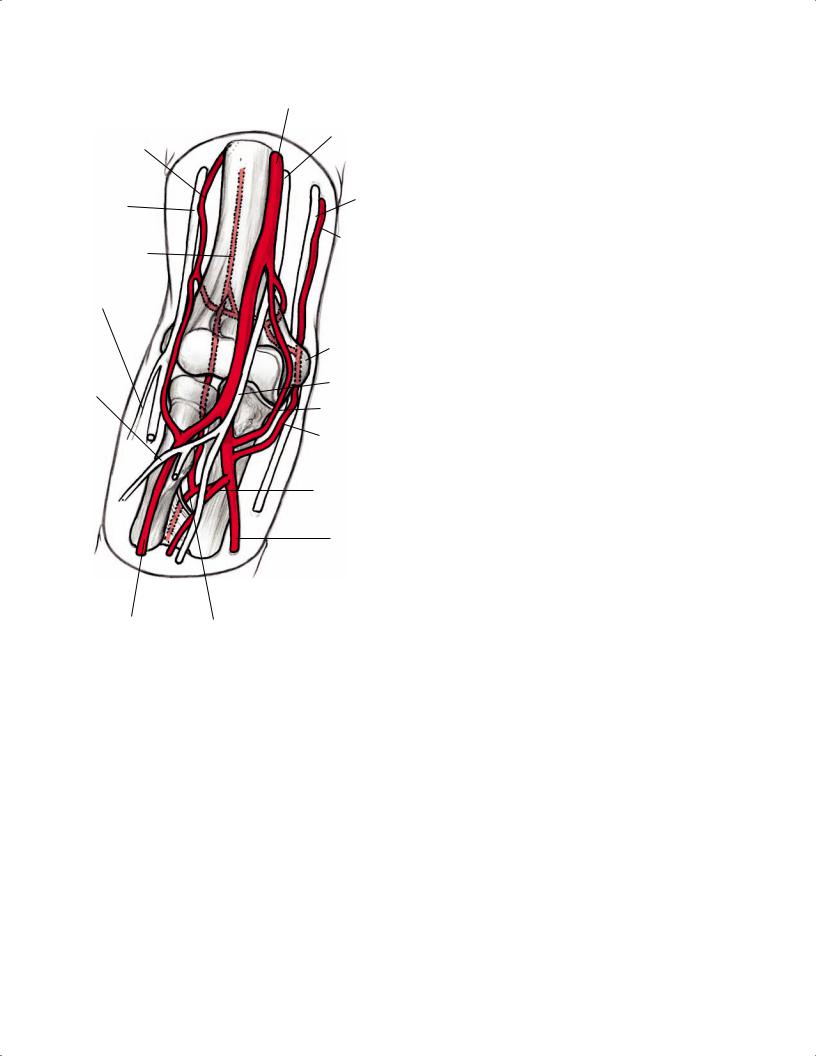
Fig. 2.15 An anterior 3D illustration of the neurovascular structures about the right elbow.
Tendons, Ligaments, and Neurovascular Structures
It is helpful to identify the origin and insertion sites of forearm tendons that involve the elbow because these locations are often the sites of tears and avulsions. Medially, the common flexor tendon is seen on axial images in cross-section as an ovoid, low signal intensity structure originating from the medial epicondyle of the humerus (Fig. 2.14). It is shared by several superficial flexor muscles in the forearm:
•Pronator teres
•Flexor carpi radialis
•Palmaris longus
•Flexor digitorum superficialis
•Flexor carpi ulnaris
•Extensor digitorum
•Extensor carpi radialis brevis
•ECU
•Extensor digiti minimi
The anconeus is fairly isolated from other musculature, located posterolateral to the elbow. Normal muscles are usually intermediate in signal intensity, so the isolation of the anconeus from other structures with similar signal intensity makes it more easily identifiable. The anconeus is a short muscle, spanning only the elbow joint, with its origin at the lateral epicondyle and its insertion along the proximal ulna. The anconeus is a weak extensor, but it also functions to tighten the joint capsule. The supinator is also seen in this general region, although it originates directly from the lateral epicondyle and the olecranon, rather than attaching to the lateral epicondyle via the common extensor tendon. The supinator runs along the radius laterally and inserts along the lateral aspect of the proximal radius.
The axial plane allows for evaluation of the neurovascular structures (Fig. 2.15). The median nerve, which lies in close association with the pronator teres and flexor carpi radialis, can often be identified as a thin, intermediate signal structure located between the ulnar and humeral heads of the pronator teres. The brachial artery, seen in close association with the origin of the pronator teres, lies lateral to the median nerve.
The ulnar nerve is well visualized posterior to the medial epicondyle within the cubital tunnel (Fig. 2.14), just deep to the cubital tunnel retinaculum, where it is surrounded by high-signal fat on non–fat-suppressed images. The ulnar nerve is normally intermediate in signal intensity. Although not present in most individuals, the anconeus epitrochlearis muscle is a normal variant structure that may overlie the
28 I Initial Concepts
cubital tunnel and ulnar nerve, extending from the posterior aspect of the medial epicondyle to the medial aspect of the ulna. Proximal to the elbow, the ulnar nerve is located along the medial border of the triceps muscle. Distal to the elbow, the ulnar nerve is seen between the two heads of the flexor carpi ulnaris muscle.
The radial nerve runs between the brachioradialis and brachialis muscles. At the level of the biceps myotendinous junction, the radial nerve can be seen dividing into its superficial and deep branches within the radial tunnel (Fig. 2.12). The posterior interosseous nerve (deep branch of the radial nerve) is located between the two origins of the supinator. The median nerve lies centrally but is di cult to distinguish from the adjacent brachial vessels.
Coronal Images
Coronal images of the elbow are obtained in a plane parallel to the interepicondylar line. Although the common flexor and common extensor tendons are seen on axial images,
these structures are also well visualized in the coronal plane. The collateral ligament complexes (Fig. 2.16) are best evaluated on coronal images. Starting with the medial aspect of the elbow, the common flexor tendon is seen as it arises from the medial epicondyle. Just deep to this tendon, the anterior band of the UCL courses from the distal margin of the medial epicondyle to its attachment on the sublime tubercle of the proximal ulna. The posterior and oblique bands of the UCL are generally not evaluated well on MRI examinations.
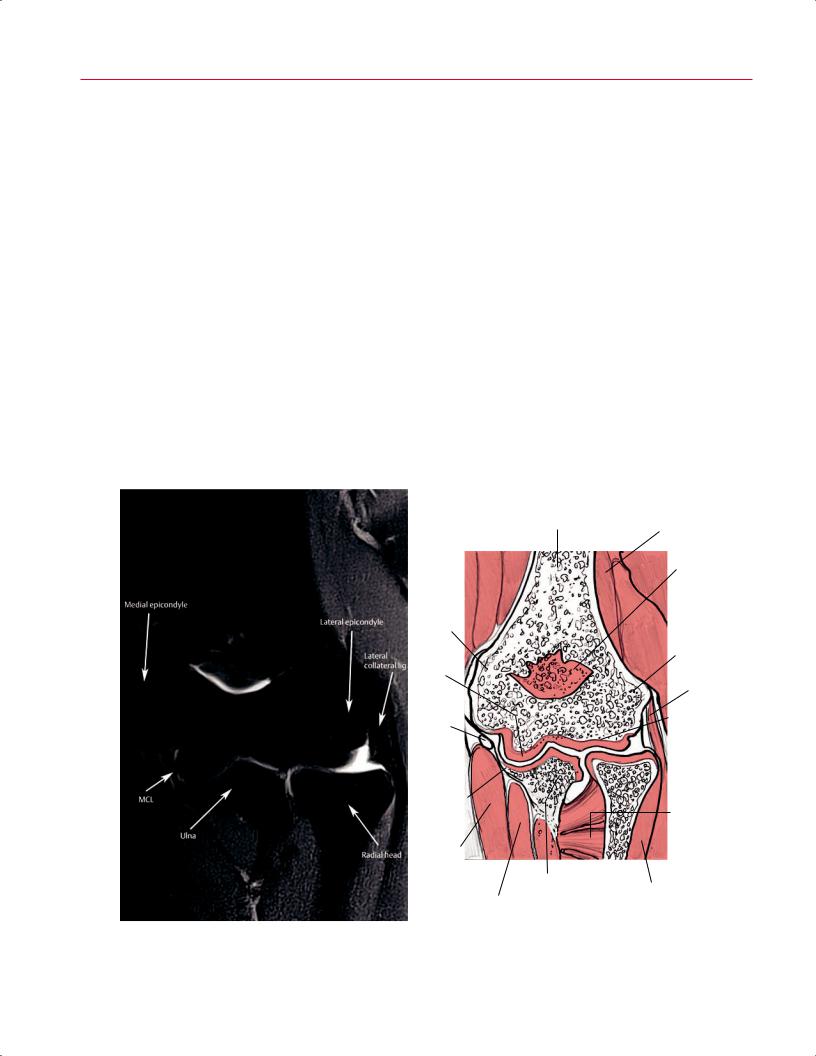
The ulnar nerve can be identified posterior to the medial epicondyle and is shown in long axis on the coronal images, allowing for large segments of the ulnar nerve to be visualized on a single image. When evaluating the lateral aspect of the elbow, the common extensor tendon can be identified arising from the lateral epicondyle of the humerus. The RCL lies deep to the common extensor tendon and extends from the anterior aspect of the lateral epicondyle to the radial head, where it inserts onto the annular ligament. The LUCL is also deep to the common flexor tendon but is more posteriorly located relative to the RCL; the LUCL extends from
Distal humerus |
Triceps m. |
|
|
Olecranon |
|
|
fossa |
|
Medial |
|
|
epicondyle |
|
|
|
Lateral |
|
|
epicondyle |
|
Trochlea |
|
|
|
|
LCL |
Ulnar n. |
Capitellum |
|
Posterior |
|
Radial |
|
head |
|
bundle of |
|
|
MCL |
Supinator |
|
|
||
|
m. |
|
Flexor |
|
|
carpi |
|
|
ularis m. |
|
|
|
|
Ulna |
||
|
|
Extensor |
||
|
Flexor digitorum |
digitorum m. |
|
|
A |
B |
|||
profundus m. |
|
|||
Fig. 2.16 A coronal proton-density fat-suppressed image (A) and artist’s sketch (B) of the left elbow showing the MCL and LCL in the long axis at the level of the radiocapitellar and ulnotrochlear articulations.
|
2 Normal MRI Anatomy of the Musculoskeletal System 29 |
||
the tubercle of the supinator crest of the ulna to the postero- |
and the accumulation of fluid in this region could be con- |
|
|
lateral aspect of the radius. The LCL complex comprises the |
fused with an OCD. Another area that may mimic a cartilage |
||
following: |
defect is along the lateral aspect of the radial head, where |
||
• RCL |
the articular cartilage is generally thinner than the cartilage |
||
in other areas of the elbow. |
|||
• LUCL |
|||
|
|
||
• Annular ligament |
Sagittal Images |
||
The articular cartilage of the radiocapitellar and ul- |
|||
notrochlear joints is well visualized in the coronal plane, |
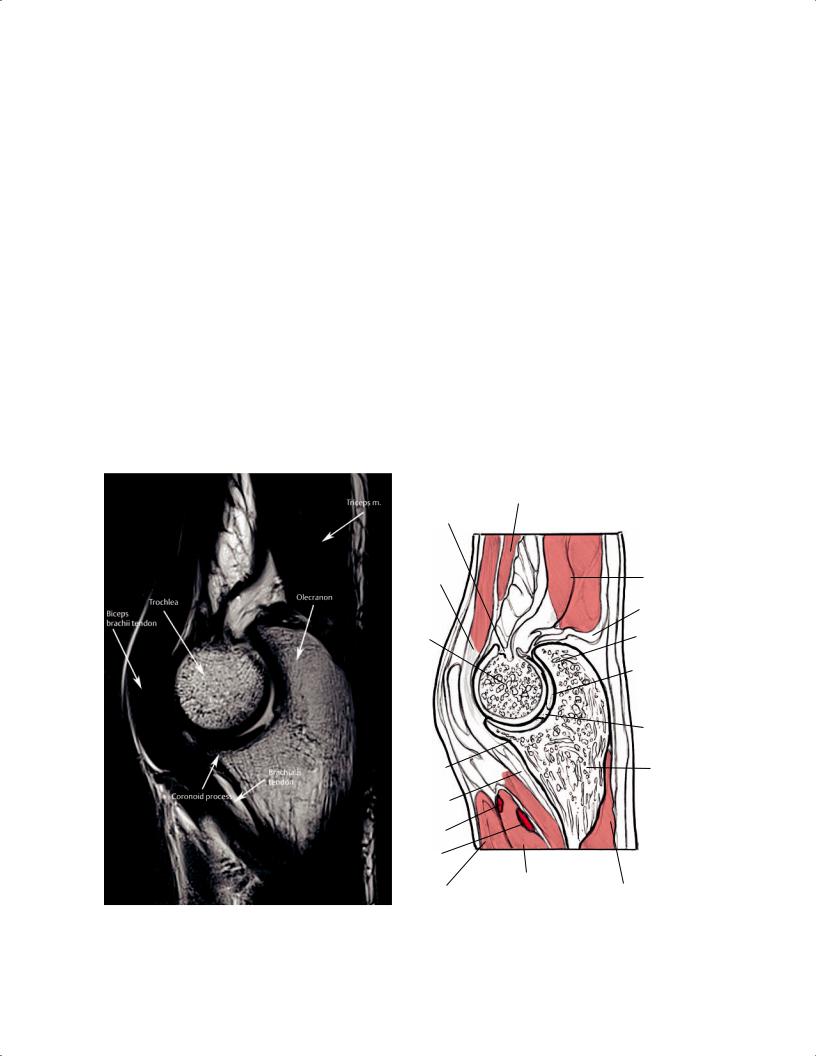
The sagittal plane is useful for evaluating osseous architecture |
||
but a “pseudodefect” is often identified on the capitellum |
and relationships, especially the humerotrochlear and radio- |
||
on more posterior coronal images. This appearance in the |
capitellar articulations (Fig. 2.17). Intraarticular bodies are |
||
coronal plane relates to the fact that the surface of the poste- |
occasionally di cult to identify because they may have signal |
||
rior capitellum is not covered with articular cartilage, often |
characteristics similar to those of joint fluid. The brachialis |
||
resulting in the appearance of a dark, thin line at the junc- |
muscle can be followed to its insertion on the ulnar tuberosity |
||
tion of the distal humerus and the capitellum; fluid accu- |
and is seen just anterior to the joint capsule. The biceps mus- |
||
mulation in this region may accentuate the appearance of a |
cle can be followed distally to its tendinous insertion on the |
||
defect because of its high signal intensity. Awareness of the |
radial tuberosity. The triceps is best seen on the midline image |
||
normal appearance of this pseudodefect is critical: the dark |
as it inserts onto the olecranon. Each of these structures can |
||
line at the junction of the distal humerus and capitellum |
usually be visualized on several images in the sagittal plane. |
||
could otherwise be misinterpreted as an impacted fracture, |
The lateral images show the components of the common |
||
|
Brachialis m. |
|
Coronoid |
|
|
fossa |
|
|
Biceps |
|
|
brachii |
Triceps |
|
tendon |
m. |
|
|
Triceps |
|
|
tendon |
|
Trochlea |
Olecranon |
|
|
Ulnohumeral |
|
|
joint with |
|
|
articular |
|
|
cartilage |
|
|
Trochlear |
|
|
groove |
|
Coronoid |
Ulna |
|
process |
||
|
Brachialis tendon
Radial a.
Ulnar a.
|
|
Pronator teres m. |
|
|
A |
Brachioradialis m. |
Flexor digitorum |
|
|
B |
||||
|
profundus m. |
Fig. 2.17 A sagittal T2-weighted image (A) and artist’s sketch (B) of the elbow showing the ulnotrochlear joint and articular cartilage, and the normal appearance of the biceps and triceps muscles in long
axis. The normal appearance of the trochlear groove as shown should not be misinterpreted as a cartilaginous defect.