


736 J.W. Lim
patient was a 11/2-year-old child with hepatocellular carcinoma who survived for a little more than 1 year before succumbing to recurrent tumor. Immunosuppression medications and surgical techniques at that time still were crude by current standards, with a dismal 1-year survival rate of 15% in 1970.
As immunosuppression (mainly the discovery of cyclosporine) and surgical technique improved from the late 1970s through the early 1980s, so did the results of liver transplants. In 1983, the National Institutes of Health (NIH) established orthotopic liver transplant (OLTX) as definitive therapy for end-stage liver disease (ESLD).1 The pioneer in OLTX has been Dr. Thomas E. Starzl. It was Starzl who, after persevering through years of experimental and clinical disappointments, paved the way for and performed the world’s first successful OLTX. It was his relentless quest for perfecting the OLTX process that led to different modalities that improved the viability of the OLTX procedure. A few of these modalities are the following2–16:
•The use of venovenous bypass to maintain systemic and splanchnic venous return in order to keep the patient hemodynamically stable during the anhepatic phase
1 National Institutes of Health (NIH) consensus statement. Liver Transplant 1983; 4(7):1–15.
2 Denmark SW, Shaw BW, Starzl TE, Griffith BP. Veno-venous bypass without systemic anticoagulation in canine and human liver transplantation. Surg Forum 1983;34:380–382. 3 Shaw BW, Martin DS, Maequez JM, et al. Venous bypass in clinical liver transplantation. Ann Surg 1984;200:524–534.
4 Griffith BP, Shaw BW, Hardesty RL, et al. Veno-venous bypass without systemic anticoagulation for transplantation of the human liver. Surg Gynecol Obstet 1985;160: 270–272.
5 Starzl TE, Marchioro TL, Porter KA, et al. The use of heterologous antilymphoid agents in canine renal and liver homotransplantation and in human renal homotransplantation. Surg Gynecol Obstet 1967;124:301–318.
6 Starzl TE, Marchioro TL, Waddell WR. The reversal of rejection in human renal homografts with subsequent development of homograft tolerance. Surg Gynecol Obstet 1963;117:385–395.
7 Starzl TE. Experience in Renal Transplantation. Philadelphia: WB Saunders, 1964.
8 Starzl TE. Immunosuppression in man. In: Starzl TE, ed. Experience in Hepatic Transplantation. Philadelphia: WB Saunders, 1969:242–276.
9 Starzl TE, Todo S, Fung J, et al. FK506 for human liver, kidney, and pancreas transplantation. Lancet 1989;2:1000–1004.
10Jamieson NV, Sundberg R, Lindell, S, et al. Successful 24to 30-hour preservation of the canine liver: a preliminary report. Transplant Proc 1988;20(suppl 1):945–947.
11Kalayoglu M, Sollinger WH, Stratta RJ, et al. Extended preservation of the liver for clinical transplantation. Lancet 1988;1:617–619.
12Todo S, Nery J, Yanaga K, et al. Extended preservation of human liver grafts with UW solution. JAMA 1989;261:711–714.
13Starzl TE, Halgrimson CG, Koep LJ, et al. Vascular homografts from cadaveric organ donors. Surg Gynecol Obstet 1979;149:737.
14Starzl TE, Miller C, Broznick B, Makowka L. An improved technique for multiple organ harvesting. Surg Gynecol Obstet 1987;165:343–348.
15Starzl TE, Demetris AJ, Van Thiel DH. Medical progress: liver transplantation, part I. N Engl J Med 1989;321:1014–1022.
16Starzl TE, Fung J, Tzakis A, et al. Baboon to human liver transplantation. Lancet 1993;341:65–71.

42. Transplantation of the Liver 737
•The use of antilymphocyte globulin (ALG), azathioprine, steroids, and, most recently, FK506 (Prograf/tacrolimus) to improve outcomes
•Improvements in preservation so as to keep the donor liver viable for a longer time
•The use of systemic arterial and venous grafts for vascular reconstruction so that those patients with abnormal or occlusive diseased anatomy also can undergo OLTX safely
•Standardizing the procurement of multiple donor organs from a single cadaver donor so as to benefit as many recipients as possible
•Discovering chimerism to explain liver tolerogenicity
Starzl has been instrumental in achieving clinical success not just in OLTX but also in kidney and intestinal transplants. It has been estimated that approximately 90% of all the transplant surgeons in the United States have been trained either directly by him or indirectly by one of his fellows.
End-Stage Complications of Liver Disease
Once patients reach ESLD, they manifest classic signs and symptoms. Clinically, these can be divided broadly into those associated with liver failure and those associated with portal hypertension (Table 42.1). These patients may have an acute process, a chronic process, a malignant process, or an inherited metabolic process that impairs the lifesustaining daily function of the native liver (Table 42.2). The end result is always death if liver failure ensues and is irreversible.
Table 42.1. Liver failure and portal hypertension in cirrhosis.
Liver failure |
Portal hypertension |
History |
History |
Fatigue |
Upper Gl variceal bleeding |
Encephalopathy |
|
Sleep–wake cycle reversal |
|
Physical exam |
Physical exam |
Jaundice |
Ascites |
Ecchymosis |
Umbilical caput medusa |
Tremor, liver flap |
Large hemorrhoids |
Gynecomastia, spider angioma |
Splenomegaly |
Testicular atrophy |
Petechiae |
Shrunken liver |
|
Laboratory exam |
Laboratory exam |
Coagulopathy |
Thrombocytopenia |
Hypoalbuminemia |
Mild neutropenia |
Elevated bilirubin |
|
Radiologic exam |
Radiologic exam |
Computed tomography: |
Ultrasound: hepatofugal portal flow |
shrunken lobulated liver |
Portal vein thrombosis |
(a cirrhotic liver may appear |
Splenic vein diameter >13 mm |
normal) |
|
Source: Reprinted from Ginns LC, Cosimi AB, Morris PJ. Transplantation. Malden, MA: Blackwell Science, Inc., 1999, with permission.

42. Transplantation of the Liver 739
treatment for HCV, including pegylated interferon and ribavirin, 20% of all patients with HCV proceed to cirrhosis. The time span to reach cirrhosis is 20 years. As cirrhosis (histopathologic diagnosis describing end-stage scarring of the liver) occurs, multiple signs and symptoms arise simultaneously, with fatigue being the most common complaint. The patient presented at the start of this chapter has some well-known risk factors for HCV; IVDA, blood transfusion, tattoos, healthcare employment, and sexual/household contact are the main risk factors. He also has classic symptoms for HCV, and his lab results are compatible with chronic HCV. A liver transplant evaluation should be part of his workup.
Transplant Evaluation
Once the patient is thought to have ESLD, ideally he/she should be referred to a liver transplant center. The liver transplant team is composed of a hepatologist, a transplant surgeon, a transplant coordinator, a social worker, and a financial coordinator. The workup focuses on identifying the cause of the ESLD and treating the symptoms and signs that have made the patient’s health deteriorate. In addition to the important history and physical, certain laboratory tests and radiologic studies are necessary to verify the disease process (Table 42.3). Once the workup is finished, the transplant team meets to review the results in order to decide if the patient is indeed a candidate and is suitable for listing, which would then place the patient on the transplant list. In general, conditions that must be met for listing to occur are the following: irreversible liver disease, stable cardiopulmonary status, no active illicit drug/alcohol abuse history, no active infection/cancer (CA) (exceptions for small-sized hepatocellular carcinomas), well-informed patient and/or family, ability to afford the medications (via insurance), and being a reasonable-risk candidate.18
Many of the acceptance criteria are similar to those for any other organ transplant candidate.
One aspect of OLTX that is very different from that of other organ transplants is that of tissue typing. For kidney transplant (K Tx), for example, data support the improved success rate with better matched donor kidneys. For kidney transplants performed between 1995 and 2001, matching at the human leukocyte antigen (HLA) -A, -B, -DR loci resulted in a 16% higher projected 10-year graft survival when compared with grafts mismatched for five or six HLAs (p < .001).19 The role of tissue typing in OLTX is minimal, and, as such, no data exist that support improved results based on matching criteria alone. As an immunologically favored organ, no crossmatch is necessary for
18 Zumeida GD, Yeo CJ. In: Turcotte JG, ed. Shackelford’s Surgery of the Alimentary Tract. Philadelphia: WB Saunders, 2002:518.
19 Ramos E, Drachenberg CB, Portocarrero M et al. BK virus nephropathy diagnosis and treatment: Experience at the University of Maryland Renal Transplant Program. In: Cecka JM, Terasaki PI, eds. Clinical Transplants 2002. Los Angeles: UCLA Immunogenetics Center, 2003:143–153.

740 J.W. Lim
patients who undergo OLTX, unlike for patients who undergo K Tx or pancreas transplant (P Tx), where a final crossmatch is warranted in almost all cases. However, just as in a K Tx and a P Tx, blood typing is mandatory, since the donor and recipient must be blood-type compatible.
Listing of Patients
The biochemical and clinical derangements that are associated with ESLD can be graded via the Child-Turcotte-Pugh (CTP) classification of hepatocellular function in cirrhosis (Table 42.4). Each designated group is assigned one, two, or three points depending on the severity. With five groups, the minimum and maximum number that can be achieved are five and 15 points, respectively. In this manner, patients are listed for OLTX only if they have at least seven points. Once the patient has been evaluated to have the indication for OLTX and after
Table 42.3. Routine liver transplantation studies.
Diagnostic studies Chest radiograph
Colonoscopy in patients with sclerosing cholangitis, history of gastrointestinal bleeding, or other specific indications
Duplex ultrasonography of hepatic vessels Electrocardiogram for those over age 40 years
Endoscopic retrograde cholangiopancreatography in patients with sclerosing cholangitis
Mesenteric angiography if duplex ultrasound is not definitive Pulmonary function testing when indicated
Ultrasound, computed tomography, or magnetic resonance imaging of liver for cirrhotics and those at risk for cancer
Upper gastrointestinal endoscopy Blood studies
ABO typing and red blood cell antibody screen
a-Fetoprotein and carcinoembryonic antigen levels for patients with cirrhosis
a1-Antitrypsin and ceruloplasmin levels in patients with cirrhosis
Arterial blood gases
Calcium and phosphorus levels Cholesterol level
Complete coagulation panel
Creatinine and blood urea nitrogen levels; creatinine clearance determination if creatinine level elevated
Glucose determination
Hematology survey, including platelet count hepatitis B and C, immunodeficiency virus, cytomegalovirus, herpes virus, varicella zoster, Epstein-Barr virus, and toxoplasmosis serology
Histocompatibility testing Liver function tests Magnesium level
Serum electrolyte levels
Total serum protein and albumin levels Uric acid determination
Source: Adapted from Zuidema GD, Yeo CJ. Shackelford’s Surgery of the Alimentary Tract. Vol III: Pancreas, Biliary Tract, Liver and Portal Hypertension, Spleen. Turcotte JG, ed. Philadelphia: WB Saunders, 2002. Copyright © 2002 Elsevier Inc. With permission from Elsevier.


742 J.W. Lim
Figure 42.1. Model for end-stage liver disease (MELD) and pediatric end-stage liver disease (PELD) mortality risks at 3 months for 1230 adult and 649 pediatric patients added to the waiting list between March 1, 2001 and August 15, 2001. (Reprinted from Freeman RB Jr, Wiesner RH, Harper A, et al. The new liver allocation system: moving toward evidence-based transplantation policy. Liver Transplant 2002;8(9): 851–858. With permission from John Wiley & Sons, Inc.)
first when there are two or more patients who have the same MELD/ PELD score and blood type.
Even with the vast majority of recipients being in critical condition just prior to transplant, the 1-year graft survival is 80.2%, with the patient survival above 86.4%.21
Contraindications
The contraindications to OLTX can be classified as being absolute and relative. As is the case with most other organ transplants, experience has led to a decreasing number of contraindications. These are noted on Table 42.5. Unlike with most other organ transplants, the psychosocial issues more often rule out a patient for transplant. This is due to the fact that the more common reason that patients require OLTX is prior illicit behavior, such as IVDA and ethyl alcohol (ETOH) abuse. Prior to the mid-1990s, ETOH was the most common reason people required OLTX. In a landmark paper from the University of Pittsburgh, Starzl reported a recidivism rate of approximately 10% posttransplant, thus putting to rest many critics who felt that an OLTX for patients with a history of ETOH abuse was not warranted.22 Most if not all centers implement a certain time frame for which the patient must be alcoholfree prior to being considered for transplant. Once listed, the recipient waits for a cadaver donor to be identified.
Donor Evaluation and Organ Procurement
The evaluation of the cadaver donor is one of the crucial steps in the success of the OLTX. Broad guidelines for acceptance criteria as a cadaver donor exist, and, as is the case for many aspects of transplant,
212002 OPTN/SRTR annual report, Table 9.9.
22Van Thiel, DH, Gavaler JS, Tarter RE, et al. Liver transplantation for alcoholic liver disease: a consideration of reasons for and against. Alcoholism Clin Exp Res 1989;13(2): 181–184.

42. Transplantation of the Liver 743
these may differ greatly from center to center (Table 42.6). In general, the cadaver donors must be deemed brain dead, most often from a cerebrovascular accident (CVA). The definition of being brain dead also may differ from hospital to hospital, but most hospitals rely on neurologic exams by two separate physicians or tests to confirm diminished blood flow to the brain. Once the donor is determined to be brain dead, laboratory tests are performed to determine the patient’s blood type and physiologically describe the patient’s body chemistry and serology. No blood work exists to reliably predict liver function in the donor and then in the recipient. A history of homosexuality or promiscuity, a history of heavy alcohol use, or a history of illicit drug abuse rules out many potential cadaver donors. Once consent is obtained from the donor’s family, the cadaver donor is taken to the operating room (OR) for a procurement, whereby transplant surgeons remove the organs to be transplanted.
In the operating room, the cadaver donor is placed under general anesthesia, and the entire abdomen and chest are prepped. An incision is made from the sternal notch to the pubic symphysis. The chest and abdomen are entered, and retractors are placed. Even if the heart and lungs are not procured, the chest is opened so as to optimize exposure of the intraabdominal organs, especially the liver. The main points of the procurement process of the liver include the following:
•Visualization of the liver, looking for sharp edges and no gross pathology
Table 42.5. Contraindications to liver transplantation.
Absolute
Advanced, uncorrectable cardiac or pulmonary disease
Severe, irreversible pulmonary hypertension Hypotension requiring vasopressor support Recent intracranial hemorrhage
Irreversible neurologic impairment HIV infection
Uncontrolled sepsis Extrahepatic malignancya
Inability to comply with posttransplant regimen Active substance abuse
Relative
Stage III or IV HCC
HBV-DNA+ and HBeAg+ hepatitis B
Cholangiocarcinoma Age over 70 years
a With the exception of skin cancer and some neuroendocrine tumors. HBeAG, hepatitis B early antigen; HBV, hepatitis B virus; HCC, hepatocellular carcinoma.
Source: Reprinted from Hanto DW, Whiting JF, Valente JF. Transplantation of the liver and intestine. In: Norton JA, Bollinger RR, Chang AE, et al, eds. Surgery: Basic Science and Clinical Evidence. New York: Springer-Verlag, 2001, with permission.

744 J.W. Lim
•Identification of any anatomic abnormalities of the liver (replaced right or left hepatic arteries exist in up to 18% of all patients)
•Control of sites for cannulation and decompression of the blood supply of the intraabdominal organs [aorta and superior/inferior vena cava (SVC/IVC)]
•Flushing of the gallbladder
•Heparinizing the donor with approximately 20,000 to 30,000 units
•Cannulating the aorta
•Infusion of University of Wisconsin solution (preservation fluid)
•Simultaneous decompression of the organs by way of incising the SVC/IVC
•Placement of ice throughout the chest and body cavity so as to better preserve the organs
If the heart is accepted, then this is the first organ to be removed, followed by the lungs. They both have the shortest cold-ischemic times, with the heart having a desired cold-ischemic time of 4 hours. Next, the liver and pancreas usually are resected en bloc and then separated on the back table. The kidneys usually are the last organs to be removed. The liver has a desired cold-ischemic time of 12 hours.
When the donor liver has been brought back to the recipient hospital, further work is performed to clean off any extraneous tissue, muscle, or lymphatics not required for the recipient operation. This is the “back-table” work, and it may take as long as an extra hour to clean up the donor liver (Fig. 42.2). Usually the recipient is brought into the operating room and prepared for OLTX simultaneously with the backtable work.
Table 42.6. Guidelines of acceptability as a cadaveric liver transplant donor.a
Age: Neonatal to 70 years of age and older No prolonged hypoxia or hypotension
No abdominal or serious systemic infection No cancer except skin or primary brain cancer
Reasonable cardiac, renal, and pulmonary function while on respirator support
Negative history for chronic liver disease and intravenous substance abuse Negative serology for human immunodeficiency virus (HIV) and syphilis No risk factors for HIV, such as intravenous drug use or prostitution Laboratory studies:b
Total bilirubin level of less than 4.0 mg/dL
Aspartate and alanine transaminase levels less than four times normal Alkaline phosphatase level less than twice normal
Prothrombin time and partial thromboplastin time no more than twice normal
Steatosis involving less than 30% to 50% of hepatocytes
a Most of these guidelines are relative, and many exceptions occur. The trend is to use higher risk donors because of the severe shortage of donor livers.
b These guidelines are relative and vary greatly among programs.
Source: Reprinted from Zuidema GD, Yeo CJ. Shackelford’s Surgery of the Alimentary Tract. Vol III: Pancreas, Biliary Tract, Liver and Portal Hypertension, Spleen. Turcotte JG, ed. Philadelphia: WB Saunders, 2002. Copyright © 2002 Elsevier Inc. With permission from Elsevier.

42. Transplantation of the Liver 745
Figure 42.2. The donor liver. A thorough understanding of the details and variations of hepatic vasculature anatomy is essential for performing the donor hepatectomy expeditiously. After the donor liver has been removed, a Javid or other suitable catheter is tied into the portal vein. This is used for flushing with University of Wisconsin preservation solution on the back table and later during implantation for infusing cold lactated Ringer’s solution containing albumin. (Reprinted from Zuidema GD, Yeo CJ. In: Turcotte JG, ed. Shackelford’s Surgery of the Alimentary Tract, vol 3: Pancreas, Biliary Tract, Liver and Portal Hypertension, Spleen. Philadelphia: WB Saunders, 2002. Copyright © 2002 Elsevier Inc. With permission from Elsevier.)
Surgical Technical Issues
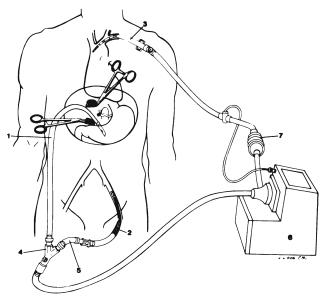
The basic technique of OLTX consists of removing the recipient’s diseased liver and replacing it with a healthy liver. The donor liver is placed in the same position as the previously removed recipient liver, and in this manner the liver transplant is termed, appropriately, orthotopic liver transplantation. Removing the diseased recipient liver is fraught with technical difficulty, since large, fragile, thin-walled veins (varices) develop around the liver substance and vascular attachments. Much blood loss can be noted during this time of the operation. To alleviate this, the concept of venovenous bypass was introduced. In this manner, direct cannulation into the systemic venous system by way of the axillary/subclavian and femoral vein and into the portal system by cannulation of the portal vein is gained (Fig. 42.3). These two systems then are connected through the bypass machine. Venovenous bypass reduces the high portal pressures seen in the varices and thereby
746 J.W. Lim
Figure 42.3. A diagrammatic representation of the venovenous bypass setup. A heparin-bonded Gott shunt is placed in the portal vein (1) and connected to a percutaneously placed femoral cannula (2) that is connected to a Bio-Medicus roller pump (6) with a flow meter (7) and heat exchanger. A return cannula is placed percutaneously into the left subclavian vein (3). (Reprinted from Johnson SR, Marterre WF, Alonso MH, Hanto DW. A percutaneous technique for venovenous bypass in orthotopic cadaver liver transplantation and comparison with the open technique. Liver Transplant Surg 1996;2:354–361. With permission from John Wiley & Sons, Inc.)
reduces the bleeding noted in the operative field. Also, because the vena cava is occluded entirely with removal of the recipient liver, the returned inferior vena caval and portal venous blood to the heart is returned via the axillary/subclavian vein cannulation. This allows placement of the donor liver and the vascular anastomoses to be performed without having to rush for fear of inhibiting inflow to the right side of the heart because of caval interruption. Once the vascular anastomoses are finished (supracaval, infracaval, portal, arterial), the biliary system is drained by way of a biliary-to-biliary or biliary-to-enteric anastomosis (Fig. 42.4).
Postoperative Complications
Complications usually result from a technical, immunologic, or infectious etiology.
The most common complication in the perioperative period is from a technical source. One of the most devastating is hepatic arterial thrombosis (HAT), which occurs in up to 5% of adults and in up to 20% of children. Often, there is no effective therapy, and the patient is relisted as a status 1 for emergent retransplantation. Other technical complications include hemorrhage, thrombosis of the vena cava or portal anastomoses, and bile duct leak or narrowing. Postoperative hemorrhage that requires reoperation for control is almost always

42. Transplantation of the Liver 747
Figure 42.4. Implantation of the donor liver. The suprahepatic vena caval anastomosis is performed first, followed by the infrahepatic vena cava, portal vein, hepatic artery, and common bile duct. (Reprinted from Hanto DW, Whiting JF, Valente JF. Transplantation of the liver and intestine. In: Norton JA, Bollinger RR, Chang AE, et al, eds. Surgery: Basic Science and Clinical Evidence. New York: Springer-Verlag, 2001, with permission.)
within the first 48 hours after the initial operation. Thrombosis of the supraor infracaval anastomosis occurs rarely, in only 1% of patients. Portal vein thrombosis has been reported to occur in as high as 10% of OLTX recipients.23,24 Biliary tract complications occur in 15% to 20% of OLTX patients, with the vast number of them occurring within the first month after surgery.25–32 The biliary complications include anastomotic
23Burke GW III, Ascher NL, Hunter D, Najarian JS. Orthotopic liver transplantation: nonoperative management of early, acute portal vein thrombosis. Surgery 1988;104:924–928.
24Davidson BR, Gibson M, Dick R, Burroughs A, Rolles K. Incidence, risk factors, management and outcome of portal vein abnormalities at orthotopic liver transplantation. Transplantation 1994;57:1174–1177.
25Colonna JO II, Shaked A, Gomes AS, et al. Biliary strictures complicating liver transplantation: incidence, pathogenesis, management, and outcome. Ann Surg 1992;216:344–352.
26Lebeau G, Yanaga K, Marsh JW, et al. Analysis of surgical complications after 397 hepatic transplantations. Surgery 1990;170:317–322.
27Stratta RJ, Wood RP, Langnas AN, et al. Diagnosis and treatment of biliary tract complications after orthotopic liver transplantation. Surgery 1989;106:675–684.
28Heffron JG, Emond JC, Whitington PF, et al. Biliary complications in pediatric liver transplantation: a comparison of reduced-size and whole grafts. Transplantation 1992;53: 391–395.
29D’Alessandro AM, Kalayoglu M, Prisch JD, et al. Biliary tract complications after orthotopic liver transplantation. Transplant Proc 1991;23:1956–1990.
30Vallera RA, Cotton PB, Clavien P-A. Biliary reconstruction for liver transplantation and management of biliary complication: overview and survey of current practices in the United States. Liver Transplant Surg 1995;1:143–152.
31Egawa H, Uemoto S, Inomata Y, et al. Biliary complications in pediatric living related liver transplantation. Surgery 1998;124:901–910.
32Greif F, Bronsther OL, Van Thiel DH, et al. The incidence/timing, and management of biliary tract complications after orthotopic liver transplantation. Ann Surg 1994;219: 40–45.
748 J.W. Lim
leaks and strictures, leaks after T-tube removal, leaks from T-tube exit sites, obstruction, and biliary fistula from stent migration.
Immunologic complications are more common after the initial hospitalization discharge. Rarely is any rejection seen in the immediate postoperative period (the so-called honeymoon phase), much as in a K Tx or a P Tx. However, up to 75% of patients will experience acute rejection after liver transplant.33 Most often, the diagnosis is made after a trend of increasing liver function studies [alanine aminotransferase (ALT) and aspartate aminotransferase (AST)] necessitates a liver biopsy. Fortunately, rejection easily is treated, and, unlike in a K Tx in which an episode of early rejection is associated with decreased long-term graft survival, this has very little bearing on OLTX long-term survival.
Infectious complications also arise after the initial perioperative period. As the immunosuppression medications make the recipient more susceptible to a whole host of infectious agents—bacterial, fungal, and viral—lifelong vigilance is a priority. Infection continues to be the leading cause of death in liver transplant patients. Overall infection rates range from 60% to 80%.34–36 Bacterial infections make up the majority of infections seen and are most common within the first month post-OLTX. Fungal infections are most commonly secondary to the Candida species and also most commonly occur within the first month post-OLTX. With respect to viral infections, much as with other organ transplants, cytomegalovirus (CMV) is the most common. Peak incidence is at 6 weeks. As a result of the high mortality associated with postoperative infections, all patients are placed on preemptive antibiotics immediately postoperatively. This often continues for many months after the initial transplant.
See Algorithm 42.1 for an algorithm for postoperative monitoring.
Immunosuppression Protocols
Although the overwhelming majority of K Tx centers use induction immunosuppression therapy for their recipients, the opposite is true for OLTX centers, where the overwhelming majority do not use induction therapy for their patients (Table 42.7). Induction therapy is defined as using polyclonal [ALG, antithymocyte globulin (ATG), thymoglobulin] or monoclonal (OKT3, Zenapax, Simulect) antibodies
33Wiesner RH, Demetris AJ, Belle SH, et al. Acute hepatic allograft rejection: incidence, risk factors, and impact on outcome. Hepatology 1998;28:638–645.
34The US Multicenter FK506 Liver Study Group. A comparison of tacrolimus (FK506) and cyclosporine for immunosuppression in liver transplantation. N Engl J Med 1994; 331:1110–1115.
35Whiting JF, Rossi SH, Hanto DW. Infectious complications after OKT3 induction in liver transplantation. Liver Transplant Surg 1997;3:563–570.
36Hadley S, Samore SH, Lewis WD, Jenkins RL, Karchmer AW, Hammer SM. Major complications after orthotopic liver transplantation and comparison of outcomes in patients receiving cyclosporine or FK506 as primary immunosuppresssion. Transplantation 1995; 59:851–859.


Lim .W.J 750
Table 42.7. Immunosuppression use for induction, 1992 to 2001: recipients with liver transplants.
|
|
|
|
|
|
Year of Transplant |
|
|
|
|
|
|
|
1992 |
1993 |
1994 |
1995 |
1996 |
1997 |
1998 |
1999 |
2000 |
2001 |
|
|
|
|
|
|
|
|
|
|
|
|
|
Transplants |
3064 |
3440 |
3652 |
3931 |
4077 |
4185 |
4503 |
4715 |
4962 |
5180 |
Tx with |
2497 |
2845 |
3093 |
3365 |
3484 |
3815 |
4083 |
4238 |
4668 |
4812 |
|
|
immunosuppression |
|
|
|
|
|
|
|
|
|
|
|
info |
|
|
|
|
|
|
|
|
|
|
No induction drugs |
99.7% |
99.3% |
87.2% |
86.2% |
90.0% |
93.0% |
91.8% |
87.4% |
84.1% |
84.8% |
|
|
recorded |
|
|
|
|
|
|
|
|
|
|
Drugs ALG |
0.0% |
0.0% |
0.0% |
0.0% |
0.0% |
— |
— |
— |
— |
— |
|
ATG |
0.2% |
0.2% |
4.3% |
4.0% |
3.6% |
2.1% |
1.1% |
0.7% |
0.6% |
0.4% |
|
NRATG/NRATS |
— |
— |
— |
— |
0.0% |
0.0% |
0.0% |
— |
0.0% |
— |
|
|
OKT3 |
0.2% |
0.5% |
8.6% |
10.0% |
6.6% |
4.9% |
3.7% |
1.5% |
0.9% |
0.7% |
|
Thymoglobulin |
— |
— |
— |
— |
— |
— |
0.1% |
0.5% |
1.2% |
2.5% |
|
Zenapax |
— |
— |
— |
— |
— |
0.0% |
2.4% |
6.2% |
6.8% |
5.9% |
|
Simulect |
0.0% |
0.0% |
0.0% |
0.0% |
0.0% |
0.0% |
1.0% |
4.1% |
6.8% |
5.9% |
ALG, antilymphocyte globulin; ATG, antithymocyte globulin; NRATG/NRATS, Nashville rabbit antithymocyte globulin/Nashville rabbit antithymocyte serum. (—), drug not used anytime during the year.
Induction drugs include any reported antilymphocyte antibodies and antibodies directed against lymphocyte receptors. Reprinted from www.transplant.org, on-line Annual Report, 2004. Source: OPTN/SRTR Data as of August 1, 2002.

42. Transplantation of the Liver 751
prior to the recipient receiving the organ. As acute rejection does not appear to have any deleterious long-term impact on graft/patient survival in the OLTX patient, most liver transplant centers have not used induction therapy with its potential to decrease acute rejection, especially in the early postoperative period.
The advent of cyclosporine (CSA) in the late 1970s markedly increased patient and graft survival, and the later discovery of Prograf/ tacrolimus (FK506) added to the improved results.37 Both drugs work to block T-cell activation primarily by inhibiting transcription of interleukin (IL)-2, IL-3, IL-4, and interferon-g (IFN-g). The newest form of CSA is Neoral and is dosed at 7 to 10 mg/kg/day in two divided doses, with a target range of 350 ng/mL. FK506 is dosed at 0.1 mg/kg/day, with a target range of 10 to 15 ng/mL.
Corticosteroids long have been part of every immunosuppression protocol for every center regardless of the organ transplanted. For many liver transplant centers, steroids now are being phased out of the protocol because of the deleterious long-term side effects associated with chronic steroid use and the better and stronger immunosuppression medications now available. One of the mainstay medications used in conjunction with Neoral or FK506 is mycophenolate mofetil (MMF). This drug blocks proliferation of T and B lymphocytes and inhibits antibody formation and the generation of cytotoxic T cells. Usually administered as 1 g twice a day, no levels are checked. Instead, doses are lowered when toxicity occurs (usually in the form of diarrhea or nausea and vomiting).
Pediatric and Living Related Liver Transplant
The indications for OLTX in children differ from the indications for OLTX in adults (Fig. 42.5). Biliary atresia usually comprises 55% to 60% of the patients who receive pediatric OLTX. Unfortunately for the pediatric recipient, finding an appropriately sized donor is more difficult, since the pediatric cadaver donor pool is far smaller than the adult cadaver donor pool. In addition, the percentage of cadaveric liver transplants going to pediatric patients decreased from 15% in 1992 to 10% in 2000.38 This is one of the reasons for the placement of the PELD score, and, in the year it was implemented, the percentage of cadaveric transplants going to pediatric recipients increased more than in any other year of the period (from 10.1% in 2000 to 10.5% in 2001).38 Also, because of the low overall number of available organs for pediatric recipients, living donor liver transplant (LDLT) was a much more common procedure in the pediatric population proportionally than in the adult population. Usually this entails taking a small piece of the liver from an adult and placing it into the child. Most often, it is
37Jain B, Hamad I, Rakela J, et al. A prospective randomized trial of tacrolimus and prednisone versus tacrolimus, prednisone, and mycophenolate mofetil in primary adult liver transplant recipients. Transplantation 1998;66:1395–1398.
38Roberts JP, Brown RS, Edwards EB, et al. Liver and intestine transplantation. Am J Transplant 2003;3(suppl 4):78–90.

752 J.W. Lim
Figure 42.5. Indications for liver transplantation in pediatric patients based on the Pitt-UNOS Liver Transplant Registry. (Reprinted from Busuttil RW, Klintmalm GB. Transplantation of the Liver. Philadelphia, W.B. Saunders Company, 1996. Copyright © Elsevier Inc. With permission from Elsevier. Data in Belle SH, Beringer KC, Murphy JB, et al. The Pitt-UNOS Liver Transplant Registry: Clinical Transplantation 1992.)
a parent-to-child donation, and, almost always, it is the left lateral segment of the left lobe of the parent that is used (Fig. 42.6). The 1-year graft and patient survival for pediatric OLTX are 81% and 89%, respectively, which are comparable to those for adult OLTX.39 As is the case in kidney transplants in children, a pediatric specialist, in this case a pediatric hepatologist, is the key to success in the overall care of the pediatric recipient. Also, as is the case for kidney transplants in children, a strong social situation is crucial to the long-term success of the transplant process. The social services evaluation is vital to obtaining the pertinent information in order to help with the decision of whether or not a pediatric recipient is a suitable candidate.
The same lengthened waiting time and the mortality rate on the adult OLTX list produced a shift toward performing more LDLT in the adult recipient population as well (Fig. 42.7). This entails taking a much bigger piece of the liver, usually the whole right lobe, from the donor and anastomosing it into the recipient. As the technical difficulty of this procedure is great, the mortality and morbidity rates are noted to be as high as 0.5% and 14.5%, respectively.40–42 Most of the compli-
392002 OPTN/SRTR Annual Report. Tables 10 and 11.
40Broering DC, Sterneck M, Rogiers X. Living donor liver transplantation. J Hepatol 2003;38:S119–S135.
41Renz JF, Roberts JP. Long-term complications of living donor liver transplantation. Liver Transplant 2000;6(6 suppl 2):S73–S76.
42Brown RS, Russo MW, Lai M, et al. A survey of liver transplantation from living adult donors in the United States. N Engl J Med 2003;348:818–825.

42. Transplantation of the Liver 753
Figure 42.6. Living related donor left lateral segment after implantation. IVC, inferior vena cava; LLHV, left lateral hepatic vein; LLBDs, segment 2 and 3 bile ducts; LPV, left portal vein; VG, vein graft; LHA, left hepatic artery; SV, saphenous vein; PV, portal vein; Ao, aorta. Inset: Final position of the graft after abdominal closure. (Reprinted from Broelsch CE, Whitington PF, Emond JC, et al. Liver transplantation in children from living related donors. Surgical techniques and results. Ann Surg 1991;214:428–439. With permission from Lippincott Williams & Wilkins.)
cations are related to the donor biliary tract system. The number of LDLTs performed has doubled in the past 2 years, and this procedure now accounts for 10% of the transplants being performed.43 Patient and graft survival for cadaver and living donor are noted in Tables 42.8 and 42.9. The trend in LDLT continues, and some have predicted that up to 30% of all OLTX will be using a living donor. As long as the shortage of donor liver organs exists, living donor and other ingenious methods to increase the donor pool will continue to evolve. Already at some
Figure 42.7. Living liver donor transplants, adults versus pediatrics, 1992– 2001. (Reprinted from 2002 OPTN/SRTR annual report.)
43 Roberts JP, Brown RS, Edwards EB, et al. Liver and intestine transplantation. Am J Transplant 2003;3(suppl 4):78–90.
754 J.W. Lim
Table 42.8. Graft survival and standard errors at 3 months, 1 year, 3 years, and 5 years; deceased donor liver transplants.
|
|
3 Months |
|
|
|
1 Year |
|
|
|
3 Years |
|
|
|
5 Years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
Std. |
|
|
|
Std. |
|
|
|
Std. |
|
|
|
Std. |
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|||||
|
n |
% |
Err. |
n |
% |
Err. |
|
n |
% |
Err. |
n |
% |
Err. |
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Total |
8735 |
85.8 |
0.4% |
8735 |
80.2 |
0.4% |
8191 |
71.4 |
0.5% |
7630 |
63.5 |
0.6% |
|||
(+), values not determined due to insufficient follow-up; (-), values not determined since there were no transplants in the category.
Cohorts are transplants performed during 1999–2000 for 3-month and 1-year survival; 1997–1998 for 3-year survival; and 1995–1996 for 5-year survival.
Graft survival follows individual transplants until graft failure. Counts for patient and graft survival are different because a patient may have more than one transplant for a type of organ.
Center volume = Center’s yearly transplants performed during the base period, based on liver transplants. Multiorgan transplants are excluded.
Reprinted from www.transplant.org, on-line Annual Report, 2004. Source: OPTN/SRTR data as of August 1, 2002.
OLTX centers, single cadaver livers are being split into two so that instead of only one recipient for every one cadaver donor, there can be two recipients. The smaller left lateral segment goes into a child or into a small recipient, and the bigger, full-sized right lobe goes into an adult or into a larger recipient.
Summary
The face of liver transplant continues to evolve as human ingenuity attempts to catch up with the persistent organ shortage. Attempts at xenotransplantation and artificial livers or assist devices still are in progress. Much research has gone into growing hepatocytes to a state that they may someday save a human life, but, to date, this still is a theory and not reality. Stem cell research at this time is still that— research without any practical current use. As more and more centers start to perform LDLT, experience will accrue and benefit future patients. Currently, with the stagnant growth in the number of cadaver donors, living donation has been the lone bright spot for all of trans-
Table 42.9. Graft survival and standard errors at 3 months, 1 year, 3 years, and 5 years; living donor liver transplants.
|
|
3 Months |
|
|
|
1 Year |
|
|
|
3 Years |
|
|
|
5 Years |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
n |
|
Std. |
|
n |
|
Std. |
|
n |
|
Std. |
|
n |
|
Std. |
|
|
|
|
|
|
|
|||||||||
|
|
|
|
|
|
|
|
||||||||
|
|
|
|
|
|
|
|||||||||
|
% |
Err. |
% |
Err. |
|
% |
Err. |
% |
Err. |
||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
Total |
605 |
83.0 |
1.6% |
605 |
76.3 |
1.8% |
170 |
72.4 |
3.5% |
109 |
73.0 |
4.4% |
|||
(+), values not determined due to insufficient follow-up; (-), values not determined since there were no transplants in the category.
Cohorts are transplants performed during 1999–2000 for 3-month and 1-year survival; 1997–1998 for 3-year survival; and 1995–1996 for 5-year survival.
Graft survival follows individual transplants until graft failure. Counts for patient and graft survival are different because a patient may have more than one transplant for a type of organ.
Center volume = Center’s yearly transplants performed during the base period, based on liver transplants. Multiorgan transplants are excluded.
Reprinted from www.transplant.org, on-line Annual Report, 2004. Source: OPTN/SRTR data as of August 1, 2002.
42. Transplantation of the Liver 755
plant, not just for OLTX. The improved results of laparoscopic donor nephrectomy have helped to increase the donor pool for the fortunate recipients with living donors. In much the same way, those patients who require OLTX and are fortunate enough to have a viable living donor now also can benefit greatly. The valuable experience of performing LDLT will only help upcoming patients. The hope is that, in the foreseeable future, LDLT will be accepted in much the same way as living donor kidney donation is accepted today.
Selected Readings
Busuttil RW, Klintmalm GB. Transplantation of the Liver. Philadelphia: WB Saunders, 1996.
Busuttil RW, Shaked A, Millis JM, et al. One thousand liver transplants: the lessons learned. Ann Surg 1994;219:490–499.
Ginns LC, Cosimi AB, Morris PJ. Transplantation. Malden, MA: Blackwell Science, 1999.
Hanto DW, Whiting JF, Valente JF. Transplantation of the liver and intestine. In: Norton JA, Bollinger RR, Chang AE, et al, eds. Surgery: Basic Science and Clinical Evidence. New York: Springer-Verlag, 2001.
Maddrey WC, Sorrell MF. Transplantation of the Liver, 2nd ed. Stamford, CT: Appleton and Lange, 1995.
Shaw BW Jr, Martin DJ, Marquez JM, et al. Venous bypass in clinical liver transplantation. Ann Surg 1984;200:524–534.
Stratta RJ, Wood RP, Langnas AN, et al. Diagnosis and treatment of biliary tract complications after orthotopic liver transplanation. Surgery 1989;106: 675–684.