

5 курс / Пульмонология и фтизиатрия / Clinical_Tuberculosis_Friedman_Lloyd_N_,_Dedicoat
.pdf130 Radiology of Mycobacterial Disease
Figure 8.2 A 43-year-old male with carpal tunnel syndrome and right paratracheal and hilar adenopathy. The carpal tunnel syndrome was the result of caseating granulomas found at surgery. In the non-HIV-positive population, adenopathy is more common in children and non-Caucasian adults, particularly in African-Americans and persons from India. Although asymmetric adenopathy is uncommon in sarcoidosis, the patterns of tuberculous adenopathy may mimic exactly those of sarcoid and lymphoma.
Figure 8.3 A 25-year-old male with fever and weight loss. The pleural effusion and adenopathy are characteristic of primary infection.
(a) |
(b) |
(c) |
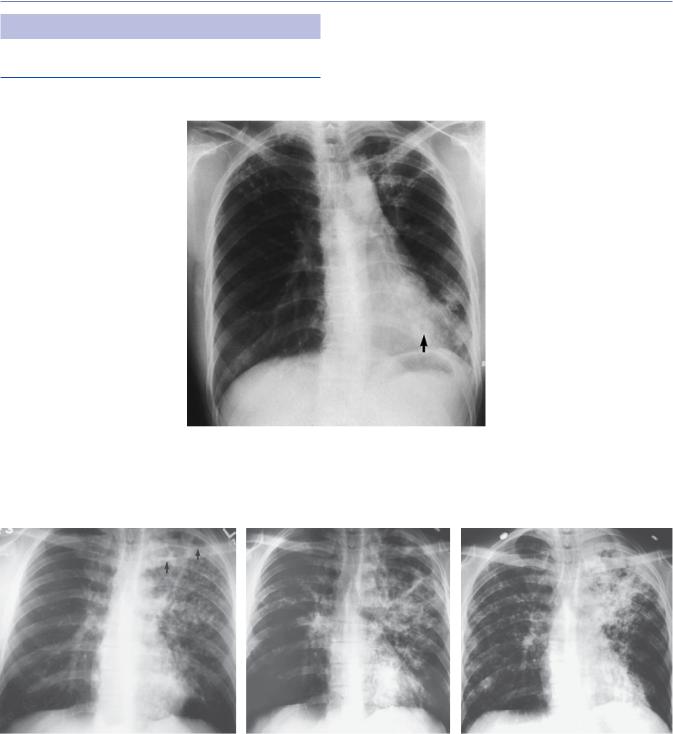
Figure 8.4 (a–c) A 40-year-old male diabetic with fever, chills, and cough of 3 weeks duration. There is an ill-defined opacity with cavitation on admission radiograph (a) (arrow), which is easily seen on computed tomography (b). A tuberculous pleural effusion developed as well (c). The patient was anergic at admission and the diagnosis was made initially by a positive smear at bronchoscopy. He then remembered that a friend had been sick with tuberculosis several months earlier (Figure 8.11 shows the contact’s films).
Книга в списке рекомендаций к покупке и прочтению сайта https://meduniver.com/

Primary tuberculosis 131
(a) |
(b) |
(c) |
(d) |
Figure 8.5 (a–d) A 25-year-old male with cough and fever. There is right paratracheal, right hilar, and aortopulmonary adenopathy as well as a left pleural effusion (b). A chest radiograph 4 months earlier (a) shows that these findings are new. All of these findings favor primary infection. The patient was lost to follow-up until he returned 2 months later with continued fever and a 30 lb. weight loss. The adenopathy and pleural effusion resolved, but there are nodules disseminated throughout both lungs (c, d); the sputum was positive for acid-fast bacilli (AFB). No apparent cavitary focus is present and the nodules, now larger than 3 mm, are too big to be considered miliary. Presumably, this represents progression of the hematogenously disseminated primary disease, or primary progressive tuberculosis.

132 Radiology of Mycobacterial Disease
(a) |
(b) |
|
(c)
Figure 8.6 (a–c) A 32-year-old male with an asymptomatic routine chest radiograph. No parenchymal focus is evident on posteroanterior and lateral chest radiographs in the presence of a large effusion (a, b). Computed tomography of the chest shows an apical focus of parenchymal disease (c). Mycobacterium tuberculosis was found on pleural biopsy and culture. In cases of pleural effusion, a parenchymal lesion that ruptures into the pleural space to produce the effusion usually may be found on computed tomography. Effusions are more frequent with primary infection.
Книга в списке рекомендаций к покупке и прочтению сайта https://meduniver.com/

Primary tuberculosis 133
Figure 8.7 A 23-year-old female, 7 weeks postpartum, presented with fever. Bilateral cavitary opacities are present in the upper lobes. The tuberculin skin test was negative and septic emboli were suspected. Angiography was negative. An open lung biopsy demonstrated M. tuberculosis. The skin test converted 6 weeks after admission.
Figure 8.8 A 32-year-old male presented with chest pain, fever, and a 20 lb weight loss the day his sister was discharged from the hospital for treatment of active pulmonary tuberculosis. Multiple areas of cavitation are noted in the left lung, which is partially collapsed in the presence of a pneumothorax. The pneumothorax probably resulted from rupture of a necrotic focus into the pleural space. Smear and culture were positive for M. tuberculosis.
(a)
(b)
Figure 8.9 (a, b) Residual pleural focus. A 45-year-old female with a history of fever and pleurisy 7 years earlier treated in China for 3 months with streptomycin, isoniazid, and penicillin. A lateral chest film and computed tomography show a pleural-based soft-tissue mass without evidence of bony destruction. No parenchymal lesions or adenopathy were evident. A needle biopsy was negative; caseating granulomas were found at surgery, and M. tuberculosis was cultured. The differential diagnosis includes pleural tumors, both benign and malignant.
134 Radiology of Mycobacterial Disease
REACTIVATION TUBERCULOSIS
Pulmonary
Figure 8.10 A 28-year-old laboratory worker with chronic cough. Bilateral upper lobe volume loss with nodular opacities of varying sizes are seen. Poorly marginated larger opacities are noted in the left lower lobe with a central lucency (arrow) representing cavitation. This is an example of bronchogenic spread.
(a) |
(b) |
(c) |
Figure 8.11 (a–c) Bronchogenic spread. A 31-year-old male with fever and cough. Cavities at the left apex (arrow) were not observed initially and the patient was treated for a presumed community acquired infection (a). Progressive cavitation developed with bronchogenic spread to both lungs (b, c). The sputum smear was markedly positive for M. tuberculosis. This patient is the contact for Figure 8.4.
Книга в списке рекомендаций к покупке и прочтению сайта https://meduniver.com/

Reactivation tuberculosis 135
(a)
(b)
Figure 8.12 (a, b) Multiple cavities with bronchogenic spread. A 52-year-old alcoholic male with cough and weight loss. The sputum smear was markedly positive for M. tuberculosis. There is extensive destruction of the right upper lobe with consolidation of the rest of the right lung and bronchogenic spread to the left lung (a). Computed tomography demonstrates much more destruction with multiple irregular cavities in the right lung, as well as tree-in-bud pattern in the left upper lobe, characteristic of bronchogenic spread (b).
Figure 8.13 Bronchogram. Extensive bronchiectasis with small cavity formation (arrows). Note the lucency peripherally which represents a cavity that did not fill (curved arrows) at bronchography. The smear was markedly positive for M. tuberculosis.

136 Radiology of Mycobacterial Disease
(a) |
(b) |
Figure 8.14 (a, b) A 60-year-old male who had had a thoracoplasty for tuberculosis 30 years earlier (a). He presented with a fever and chest radiograph shows miliary dissemination (b).
(a) |
(b) |
Figure 8.15 (a, b) A 55-year-old female with diabetes who underwent a therapeutic pneumothorax for tuberculosis in 1944. Multiple complications followed a coronary artery bypass graft in October 1991 (a). In January 1992, the patient developed a relentless fever and the sputum was positive for M. tuberculosis. On the film of January 1992 (b), lucencies in the left upper lobe represent necrotic foci from which bronchogenic spread occurred (arrow).
Figure 8.16 Tree-in-bud pattern. A 31-year-old Asian female presented with cough, fever, and a positive smear for M. tuberculosis. The buds, or tufts (small arrowhead), represent impacted material in the lobular bronchioles and alveolar ducts, while the stem represents impaction in the last order bronchus of the secondary pulmonary lobule (large arrowhead).
Книга в списке рекомендаций к покупке и прочтению сайта https://meduniver.com/

Reactivation tuberculosis 137
Extrapulmonary
(b)
(a)
Figure 8.17 (a, b) A 43-year-old male with multiple abdominal fistulae and abscesses as a result of a gunshot wound. One year following the initial injury, he developed miliary lesions in the lung. Bronchoscopy demonstrated caseating granulomas, M. tuberculosis was grown from the lungs, and multiple abscesses were visualized in the abdomen. Miliary lesions are seen on a chest radiograph (a) and to better advantage on computed tomography (b).
(a) |
(b) |
Figure 8.18 (a, b) A 50-year-old female with a history of congestive heart failure and hip pain who was treated with steroids. The chest radiograph initially was thought to suggest congestive heart failure (a). However, typical miliary lesions are noted throughout both lungs. Such miliary spread may occur either in primary or reactivation tuberculosis. The left hip film demonstrates narrowing and destruction of the joint space (arrows) (b). Lack of marginal erosions of the joint are unusual. Aspiration of the hip demonstrated M. tuberculosis. Presumably, the steroids led to the breakdown of preexisting tuberculous foci.

138 Radiology of Mycobacterial Disease
(a) |
(b) |
Figure 8.19 (a, b) Progressive fibrothorax. A fibrothorax resulting from a tuberculous empyema is shown with progressive contraction and calcification of the left pleural space over 26 years. Computed tomography occasionally may demonstrate fluid within the “fibrothorax” and viable organisms may be present as well, predisposing to reactivation. Hydropneumothorax (b) resulted from attempted aspiration.
(b) |
(c) |
(d) |
(a)
Figure 8.20 (a–d) A 35-year-old female with cough. A chest radiograph in May 1983 demonstrates right paratracheal adenopathy (a). A barium swallow shows ulceration of the esophagus with extravasation of contrast into the tracheobronchial tree at the level of the subcarinal lymph nodes (arrows) (b, c). Follow-up in October demonstrates healing with a residual esophageal diverticulum (arrows) (d). Similar pathology with erosion of tuberculous nodes into the right middle lobe bronchus with resulting stricture was the original cause of the right middle lobe syndrome, i.e., atelectasis with a patent bronchus.
Книга в списке рекомендаций к покупке и прочтению сайта https://meduniver.com/

Healing 139
(b)
(a)
Figure 8.21 (a, b) Tuberculosis of the spine and cavitary tuberculosis of kidney. Destruction of the inferior portion of an upper thoracic vertebral body and complete destruction of the vertebral body below resulted in a gibbus deformity (a). The initial infection usually results from hematogenous spread. Spread from one vertebral body to the next may occur across the disk space or beneath the anterior and posterior longitudinal ligaments. The cavitary lesions in the kidney (arrows) are filled with debris (b). Stricture formation may occur with healing, and careful follow-up with intravenous pyelography is warranted to avoid obstruction. (Photo courtesy of Arthur Rosenfield, MD.)
HEALING
Figure 8.22 Formation of Rhanke complex. Calcified nodule associated with a calcified mediastinal lymph node.