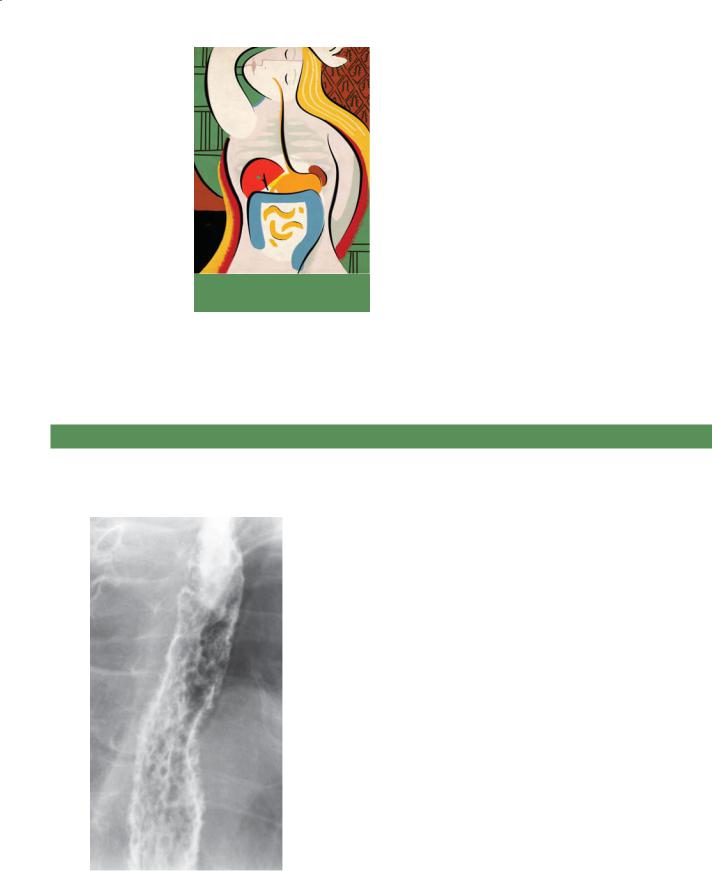
11.1. Which of the following is the most likely diagnosis for the findings shown in the figure?
a.Candidiasis
b.Herpes esophagitis
c.Cytomegalovirus (CMV) esophagitis
d.Human immunodeficiency virus (HIV) esophagitis
e.Refl ux esophagitis
858 MAYO CLINIC GASTROINTESTINAL IMAGING REVIEW
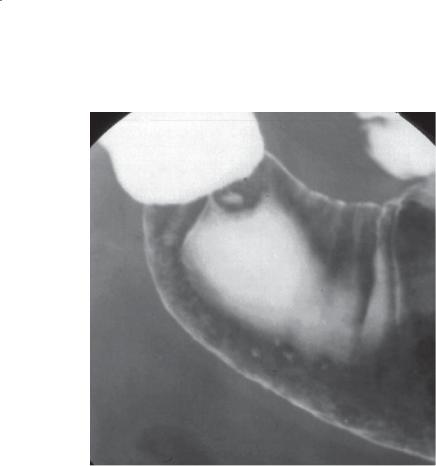
11.2. Which of the following is the most likely diagnosis for the findings shown in the figure?
a.Normal pyriform sinuses
b.Vallecular neoplasm
c.Pharyngeal pouch
d.Zenker diverticulum
e.Killian-Jamieson diverticulum
11. FINAL EXAMINATION 859
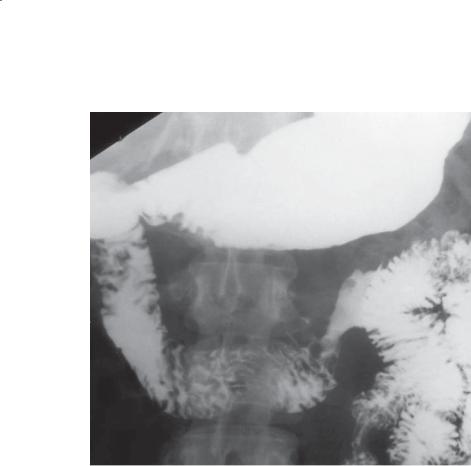
11.3. What is the most common cause for the condition shown in the figure?
a.Radiation therapy
b.Crohn disease
c.Sarcoidosis
d.Nonsteroidal anti-inflammatory drug
e.Acid ingestion
860 MAYO CLINIC GASTROINTESTINAL IMAGING REVIEW
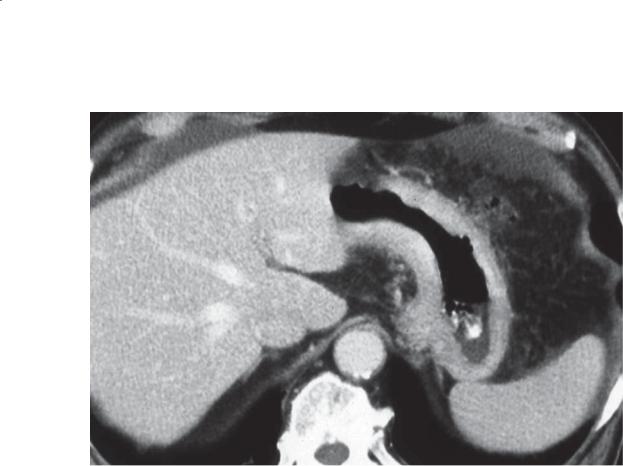
11.4. Which of the following differential pairs is most likely for the findings shown in the figure?
a.Gastritis and cancer
b.Helicobacter pylori infection and underdistention
c.Primary gastric cancer and metastases
d.Radiation gastritis and cancer
e.Crohn disease and underdistention
11. FINAL EXAMINATION 861
11.5. How is the condition shown in the figure usually treated?
a.Whipple procedure
b.Simple surgical resection
c.No treatment usually necessary
d.Proton pump inhibitor
e.Immunosuppression
862 MAYO CLINIC GASTROINTESTINAL IMAGING REVIEW
11.6. Which of the following is the most likely diagnosis for the findings shown in the figure?
a.Sprue
b.Zollinger-Ellison syndrome
c.Primary duodenal carcinoma
d.Crohn disease
e.Brunner gland hyperplasia
11. FINAL EXAMINATION 863
11.7. What other findings are often associated with the condition shown in the figure?
a.Liver abscess
b.Fibrofatty mesenteric proliferation
c.Ectopic gastric mucosa
d.Ovarian tumors
e.Ampullary neoplasm
864 MAYO CLINIC GASTROINTESTINAL IMAGING REVIEW
11.8. Which of the following is the most likely diagnosis for the findings shown in the figure?
a.Ischemic bowel
b.Closed loop obstruction
c.Crohn disease
d.Small bowel diverticulitis
e.Cirrhosis with small bowel congestion and ascites
11. FINAL EXAMINATION 865
11.9. In this figure, from a patient who recently received treatment for diverticulitis, what is the most likely cause for the condition shown?
a.Anticoagulation
b.Antibiotics
c.Constipation
d.Atrial fi brillation
e.Recurrent diverticulitis
866 MAYO CLINIC GASTROINTESTINAL IMAGING REVIEW
11.10. Which of the following is the most likely diagnosis for the findings shown in the figure?
a.Endometriosis
b.Ischemic bowel
c.Meckel diverticulum
d.Peritoneal metastasis
e.Diverticulitis
11. FINAL EXAMINATION 867
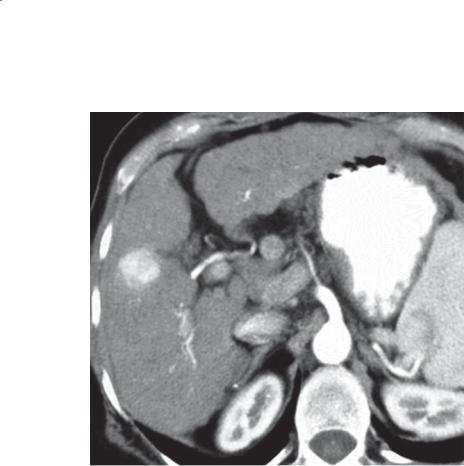
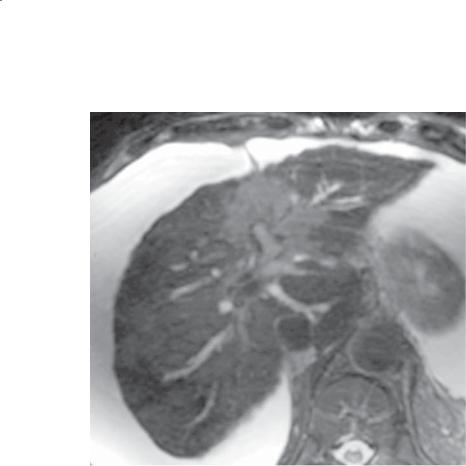
11.11. Which of the following is the most likely diagnosis for the findings shown in the figure?
a.Focal nodular hyperplasia
b.Cavernous hemangioma
c.Hepatic adenoma
d.Hepatocellular carcinoma
e.Hypervascular metastasis
868 MAYO CLINIC GASTROINTESTINAL IMAGING REVIEW
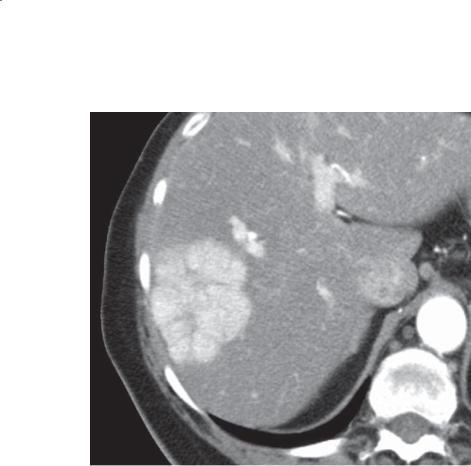
11.12. Given the findings in the figure, what is the next best study to confirm the diagnosis?
a.Serum α-fetoprotein
b.Gadoxetate delayed MRI
c.Delayed CT
d.Inand out-of-phase MRI
e.Diff usion MRI
11. FINAL EXAMINATION 869
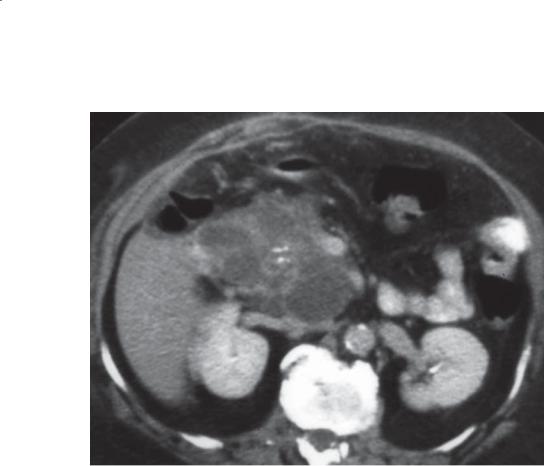
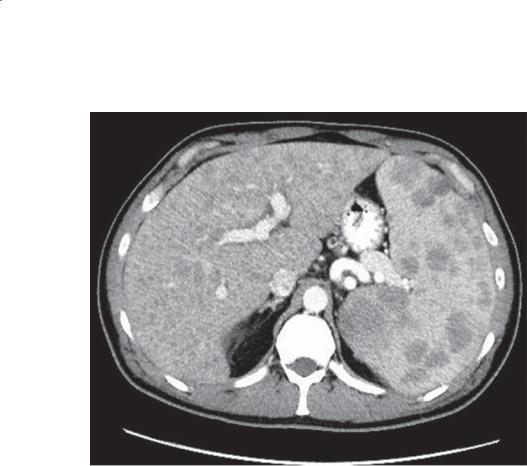
11.13. What other radiologic finding is most likely to be identified in patients with the condition shown in the figure?
a.Solitary gastric varices
b.Solid renal neoplasm
c.Primary tumor in the colon
d.Pseudoaneurysm of the splenic artery
e.Pancreatic divisum
870 MAYO CLINIC GASTROINTESTINAL IMAGING REVIEW
11.14. Which of the following is the most likely diagnosis for the findings shown in the figure?
a.Mucinous cystadenocarcinoma
b.Serous cystadenoma
c.Pseudoaneurysm
d.Pseudocyst
e.Biliary cystadenoma
11. FINAL EXAMINATION 871
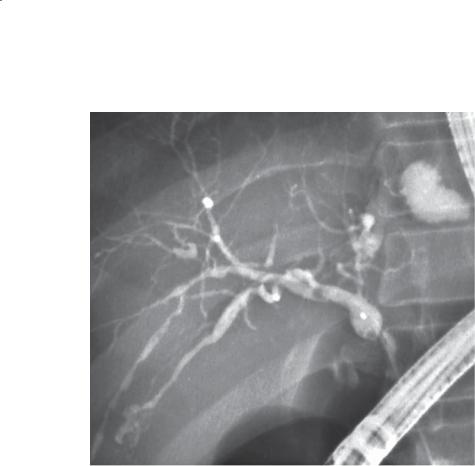
11.15. Which of the following is the most likely diagnosis for the findings shown in the figure?
a.Choledochal cyst
b.Oriental cholangiohepatitis
c.Primary sclerosing cholangitis
d.Cholangiocarcinoma
e.Primary biliary cirrhosis
872 MAYO CLINIC GASTROINTESTINAL IMAGING REVIEW
11.16. Which of the following diseases is most commonly associated with the condition shown in the figure?
a.Cirrhosis
b.Colon cancer
c.Ulcerative colitis
d.Lung cancer
e.Porcelain gallbladder
11. FINAL EXAMINATION 873
11.17. Which of the following is the most likely diagnosis for the findings shown in the figure?
a.Mesothelioma
b.Peritonitis
c.Retractile mesenteritis
d.Omental infarction
e.Omental carcinomatosis
874 MAYO CLINIC GASTROINTESTINAL IMAGING REVIEW
11.18. What is the most appropriate treatment for the condition shown in the figure?
a.Surgical removal
b.Conservative therapy
c.Embolization
d.Chemotherapy
e.No treatment is required
11. FINAL EXAMINATION 875
11.19. Which of the following is the most likely diagnosis for the findings shown in the figure?
a.Candidiasis
b.Sarcoidosis
c.Hemangiomatosis
d.Epidermoid cysts
e.Lymphoma
876 MAYO CLINIC GASTROINTESTINAL IMAGING REVIEW
ANSWERS
11.1.Answer a.
Multiple filling defects are throughout the esophagus. All of the other conditions listed present with ulcerations with collections of barium. Herpes presents with multiple discrete ulcers, CMV and HIV present with solitary and large ulcers, and reflux presents with a few ulcers in the distal esophagus with fold thickening.
11.2.Answer d.
Th ere is a prominent cricopharyngeus muscle (cricopharyngeal bar) with a diverticulum that protrudes inferior to the muscle and posterior to the esophagus. Killian-Jamieson diverticula arise below the cricopharyngeus muscle laterally.
11.3.Answer d.
Nonsteroidal anti-inflammatory drugs and Helicobacter pylori infection are commonly associated with superficial gastric erosions. Multiple tiny collections of barium are present in the antrum of the stomach, and a uniform mound of edema surrounds the tiny ulceration.
11.4.Answer c.
Th ere is uniform, enhanced thickening of the gastric wall. Differential considerations should include primary scirrhous carcinoma of the stomach and metastatic breast cancer. These infiltrative tumors can give the appearance of underdistention, but the lumen is nearly all gas-filled. H pylori infection and gastritis are associated with fold thickening and ulceration, usually in the antrum. Crohn disease usually affects the antrum, usually with other affected areas.
11.5.Answer b.
Th e figure shows an intraluminal duodenal diverticulum causing a windsock deformity within the descending duodenum. This can present with symptoms that mimic peptic ulcer disease, pancreatitis, or obstruction. Usually, surgical incision and resection are performed for treatment.
11.6.Answer c.
A focal area of ulceration (normal folds are absent), luminal narrowing, and abrupt edges are within the fourth portion of the duodenum. The appearance and location are typical of a primary duodenal adenocarcinoma.Metastaticdiseaseorpancreaticcancer could present with these findings. Zollinger-Ellison syndrome is usually associated with hypersecretion and thick gastric folds. Sprue can present with a dilated duodenum with thickened folds (megaduodenum). Crohn disease usually presents with a long segment of involvement, involvement elsewhere in the small bowel
(ileum), and nodular fold thickening. Brunner gland hyperplasia presents with multiple filling defects in the proximal duodenum.
11.7.Answer b.
Th is patient with Crohn disease has ileal wall thickening and mucosal hyperenhancement. Fibrofatty mesenteric proliferation is a commonly identified abnormality in patients with Crohn disease. Liver abscess could be found in a patient with diverticulitis or amebiasis. Ectopic gastric mucosa is found in a Meckel diverticulum. Ovarian tumors can be found with a gastric malignancy (Krukenberg tumor). Ampullary neoplasms can occur in patients with familial polyposis syndrome.
11.8.Answer a.
Th is is a case of ischemic bowel due to mesenteric vein thrombosis. A single small bowel loop is thickened with water attenuation bowel wall (edema). There is fluid within the mesentery and a small amount of ascites. The affected small bowel loop does not enhance as well as other small bowel, and the mesenteric veins and superior mesenteric vein are hypoattenuating. No twisting or entrance-exit loop is present for closed loop obstruction. Crohn disease has hyperattenuating bowel with acute inflammation. Cirrhosis does not cause differential bowel perfusion. Diverticulitis is rare in the small bowel, and there are usually more peribowel inflammatory changes without vascular findings.
11.9.Answer b.
Antibiotics can cause pseudomembranous colitis. The colon is dilated throughout with diffusely thickened folds. The findings are those of an acute colitis. The differential considerations include inflammatory bowel disease, pseudomembranous colitis, ischemic colitis, or an infectious colitis. With the history of recent treatment of diverticulitis, antibiotic therapy would usually be used. Pseudomembranous colitis is a wellknown complication of antibiotic therapy. Hemorrhage into the wall of the colon from anticoagulants would not involve the entire colon. Constipation does not cause an acute colitis. Atrial fibrillation with an embolus usually involves only a segment of bowel, not the distribution of the superior and inferior mesenteric arteries combined (pancolitis). Recurrent diverticulitis does not cause an acute pancolitis.
11.10.Answer e.
Classic findings of diverticulitis are present with bowel wall thickening, perisigmoidal soft tissue thickening,
11. FINAL EXAMINATION 877
and an adjacent pericolonic fluid collection containing a tiny air bubble (abscess).
11.11.Answer d.
Th e liver has a nodular contour, an indication of cirrhosis. A focal solid mass in a cirrhotic liver should be considered hepatocellular carcinoma until proved otherwise. Delayed imaging would be helpful to assess for washout (hypoattenuating compared with liver) in hepatocellular carcinomas because of the arteriovenous shunting that is usually present.
11.12.Answer b.
Th e mass has a scalloped border, central scar, and septations. There is homogeneous enhancement of the lesion during the arterial phase at CT. These features are characteristic of focal nodular hyperplasia. The best confirmatory test (if required) is the administration of gadoxetate, a hepatobiliary MRI contrast agent that is taken up in the vast majority of patients with focal nodular hyperplasia. Delayed imaging is usually required to visualize the uptake of the agent.
11.13.Answer a.
Th is patient has a typical pancreatic cancer with a hypoattenuating mass in the body of the pancreas and multiple hepatic metastases. Pancreatic cancer and pancreatitis are common causes of splenic vein occlusion. Splenic vein occlusion results in gastric varices and upper abdominalvariceswithoutesophagealvarices.Solidrenal neoplasms in von Hippel-Lindau disease are associated with serous cystadenomas and islet cell tumors of the pancreas. Colon cancers do not usually metastasize to the pancreas. Pseudoaneurysms and pancreatic divisum are associated with acute pancreatitis.
11.14.Answer b.
Th is large cystic mass in the pancreatic head has multiple cystic compartments, most less than 2 cm in diameter. There is central calcification, and the septations are smooth with nodularity. These findings are typical of a serous cystadenoma of the pancreas. Mucinous neoplasms can present as a solitary cyst (or few cysts), main duct dilatation, or side branch dilatation (multiple). Biliary cystadenomas are usually in the liver, arising from the bile ducts. Pseudoaneurysms usually are associated with a dilated artery. Pseudocysts usually do not have the many internal septations found with central calcifications (whereas this mass has structured internal contents favoring a tumor).
11.15.Answer c.
Th e bile ducts have an irregular dilatation and narrowing typical for primary sclerosing cholangitis.
Some of the ducts are quite dilated, an indication of higher-gradeobstruction.Choledochalcyststhatinvolve the intrahepatic ducts (Caroli disease) usually present with focal areas of dilatation without biliary strictures. Oriental cholangiohepatitis usually is associated with multiple filling defects due to stones and debris upstream from a stricture(s). Cholangiocarcinoma usually presents as a central mass with a dominant stricture at ERCP. Primary biliary cirrhosis usually has uniform-caliber bile ducts, but they are tortuous as a result of the shrunken, cirrhotic liver.
11.16.Answer c.
Th ere is a central high-intensity mass within the liver with associated bile duct dilatation to the level of the mass. These findings are consistent with a malignancy, and its central location and biliary obstruction favor a cholangiocarcinoma. Cholangiocarcinomas can arise without a preexisting disease but are associated with primary sclerosing cholangitis and choledochal cysts. Many patients with primary sclerosing cholangitis have ulcerative colitis. Colon cancer and lung cancer could present in this fashion, but usually multiple lesions are found throughout the liver. Porcelain gallbladder predisposes to gallbladder cancer.
11.17.Answer e.
Th ere is soft tissue within the omentum, known as an omental cake. Mesothelioma can present similarly, but usually there is even more involvement of the mesenteric leaves (it is also less common). Peritonitis would thicken theenhancingperitoneum.Retractilemesenteritisinvolves the mesentery primarily, not the omentum. Omental infarction presents as a discrete rounded mass in the anterior abdomen with soft tissue stranding and internal fat. Soft tissue nodules are not present in infarction.
11.18.Answer a.
Th ere is a mixed-attenuation, well-circumscribed mass in the anterior abdomen containing air and fluid. This is a typical appearance of a gossypiboma from a retained surgical towel. It must be removed surgically because it will become infected.
11.19.Answer e.
Th ere are multiple moderate-sized filling defects within the liver and spleen. The findings are due to lymphoma. Candidiasis causes smaller water-attenuation lesions in the liver and spleen. Sarcoidosis could have this appearance, but it is much less likely. Hemangiomas can be multiple but have globular blood-density enhancement. Epidermoid cysts are usually solitary benign-appearing cysts and do not involve the liver.