


Chapter 22 |
653 |
|
|
Urogynaecology
Classification of urinary incontinence 654 Urinary symptoms 655
Assessment of the lower urinary tract: history and examination 656
Assessment of the lower urinary tract: investigations 658 Assessment of the lower urinary tract: imaging 659 Assessment of the lower urinary tract: urodynamic
investigations 660
Stress urinary incontinence: overview 663
Stress urinary incontinence: conservative management 664 Stress urinary incontinence: surgical management 666 Overactive bladder syndrome: overview 668
Overactive bladder syndrome: management 670 Anatomy of the pelvic floor 672
Prolapse: classification 674 Prolapse: clinical assessment 676
Prolapse: conservative management 678
Prolapse: surgical management, anterior and posterior compartments 680
Prolapse: surgical management, uterovaginal and vault 682


URINARY SYMPTOMS 655
Urinary symptoms
•Urinary incontinence: is the complaint of involuntary urinary leakage, which can be divided, broadly, into stress incontinence and urge incontinence.
•Daytime frequency: the number of times a woman voids during waking hours—normally between 4 and 7 voids/day. Increased daytime frequency is when a woman perceives she voids too often.
•Nocturia: the complaint of having to wake at night one or more times to void. Up to the age of 70yrs, more than a single void is considered abnormal.
•Nocturnal enuresis: urinary incontinence occurring during sleep.
•Urgency: sudden compelling desire to pass urine, which is difficult to defer. Urgency is most frequently sto detrusor overactivity, although inflammatory bladder conditions such as interstitial cystitis may also present with this.
•Voiding difficulties include:
•hesitancy (difficulty in initiating micturition)
•straining to void
•slow or intermittent urinary stream.
These are all suggestive of urethral obstruction, underactive detrusor muscle, or loss of coordination between detrusor construction and urethral relaxation. Intermittency is seen with neurological disease.
•Post-micturition symptoms include:
•feeling of incomplete bladder emptying
•terminal dribble (a prolonged final part of micturition)
•post-micturitional dribble (the involuntary loss of urine immediately after passing urine).
•Absent or reduced bladder sensation: usually due to denervation caused by spinal cord injuries or pelvic surgery. Leads to infrequent micturition and large-capacity bladder, and is often associated with overflow incontinence.
•Bladder pain: felt suprapubically or retropubically. Typically occurs with bladder filling and is relieved by emptying it. Pain is indicative of intravesical pathology, such as interstitial cystitis or malignancy, and warrants further investigation.
•Urethral pain: felt in urethra (the woman indicates this as the site of the discomfort).
•Dysuria: pain experienced in bladder or urethra on passing urine. Most frequently associated with urinary tract infections.
•Haematuria: presence of blood in urine; can be microor macroscopic (frank). Always significant and warrants further investigation.
656 CHAPTER 22 Urogynaecology
Assessment of the lower urinary tract: history and examination
History
•The onset of urinary symptoms, their duration, and their severity should be recorded (the predominant bother symptom, e.g. urgency, urge incontinence, or stress incontinence, should be identified).
•Different underlying conditions can cause similar urinary symptoms; history alone is often a poor predictor of pathophysiology.
•Check for coexisting medical conditions and optimize their treatment (the onset of diabetes significantly increases urine output and many pharmaceutical agents can alter bladder function).
•Enquire about colorectal symptoms and genitourinary prolapse.
Quality of life assessment
•A good clinical history will enquire how symptoms affect aspects of daily life and social, personal and sexual relationships.
•Disease-specific QoL questionnaires allow in-depth assessment of the impact-specific symptoms on a woman’s life: validated questionnaires are available from the International Consultation on Incontinence (M www.iciq.net).
Frequency/volume chart
•The frequency/volume chart (Fig. 22.1) is a simple and practical method of obtaining objective quantification of fluid intake and voiding behaviour.
•Fluid intake, frequency, times of voiding, and leakage episodes (day and night) are recorded for at least 24h (typically 3 days).
Physical examination
General examination
•Weight (BMI), BP, urinalysis.
•Check for signs of systemic disease.
•Mobility and mental state.
•Motivation and manual dexterity.
•Neurological examination, if there are any symptoms that point to a possible neurological cause.
Abdominal examination
•Exclude an abdominal or pelvic mass (1including pregnancy).
•Exclude a full bladder (obstruction/retention).
Pelvic examination
•Condition of the vulval skin (any atrophy, erythema, or oedema).
•Presence and degree of any concurrent uterovaginal prolapse.
•Assessment of urethral and bladder neck descent on straining.
•Assessment of pelvic floor muscle strength (graded 0–5 on a modified Oxford scale; see bProlapse: clinical assessment, p. 676).

ASSESSMENT OF THE LOWER URINARY TRACT HISTORY 657
Frequency/Volume Chart
Name: Mrs Smith Patient No. 1234567 Week commencing 26 Jan 2006
Time |
Date:26.01.06 |
Date:27.01.06 |
Date:28.01.06 |
||||||
|
|
Day 1 |
|
|
Day 2 |
|
|
Day 3 |
|
am |
In |
Out |
Wet |
In |
Out |
Wet |
In |
Out |
Wet |
1 |
|
300 |
X |
|
500 |
X |
|
|
|
2 |
|
300 |
X |
|
|
|
|
|
|
3 |
|
|
|
|
600 |
X |
|
700 |
X |
4 |
|
350 |
X |
|
|
|
|
|
|
5 |
|
|
|
|
|
|
|
|
|
6 |
|
|
|
|
600 |
X |
|
600 |
X |
7 |
|
500 |
X |
|
|
|
|
|
|
8 |
|
|
|
250 |
300 |
|
|
500 |
X |
9 |
250 |
300 |
|
200 |
|
|
250 |
|
|
10 |
|
|
|
|
|
|
|
300 |
|
11 |
|
|
|
|
|
|
200 |
|
|
12 |
|
|
|
200 |
|
|
|
100 |
|
pm |
|
|
|
|
|
|
|
|
|
1 |
200 |
100 |
|
|
100 |
|
|
|
|
2 |
|
|
|
|
|
|
200 |
300 |
|
3 |
|
|
|
|
|
|
|
|
|
4 |
|
|
|
200 |
|
|
|
|
|
5 |
250 |
120 |
|
|
|
|
|
200 |
|
6 |
|
|
|
|
|
|
200 |
|
|
7 |
|
|
|
200 |
100 |
|
|
|
|
8 |
|
|
|
|
|
|
|
|
|
9 |
|
200 |
|
|
100 |
|
|
|
|
10 |
|
|
|
|
|
|
|
|
|
11 |
|
100 |
|
|
200 |
|
200 |
200 |
|
12 |
|
|
|
|
|
|
|
|
|
Total |
650 |
2270 |
|
1050 |
2500 |
|
1050 |
2800 |
|
Fig. 22.1 A 3-day frequency/volume chart showing severe nocturia.
Information obtainable from a frequency/volume chart
•Functional bladder capacity.
•Volumetric summary of diurnal urinary frequency.
•Volumetric summary of nocturnal urinary frequency.
•Quantification of total fluid intake.
•Distribution of fluid intake throughout the day.
•Total voided volume and diurnal distribution of voiding.
•Evaluation of the severity of urinary incontinence.

658 CHAPTER 22 Urogynaecology
Assessment of the lower urinary tract: investigations
Basic investigations
Urinalysis
Reagent strip testing of urine for leucocyte esterase, nitrites, protein, blood, and glucose is a sensitive and cheap screening test.
Urine specimen
Bacteriological analysis of a midstream urine specimen for microscopy, culture, and sensitivity is reserved for those with a positive screening test.
Residual check
A post-void residual check should be carried out (either by USS or by catheterization) to exclude incomplete bladder emptying.
Pad test
This is a simple method of detecting and quantifying urinary leakage based on weight gain of absorbent pads during a set period of time.
2It is not helpful in determining the cause of urinary leakage.
Cystourethroscopy
•Allows visualization of all the lower urinary tract: urethra, bladder mucosa, trigone, and ureteric orifices.
•Can be performed using a rigid or flexible cystoscope, with or without anaesthesia.
•Bladder biopsies can be taken to obtain histological diagnosis and exclude malignancy.
•In cases of suspected interstitial cystitis a second-look cystoscopy should be performed after the initial bladder distension, to detect any glomerulations or petechial haemorrhages.
Indications for cystourethroscopy
•Recurrent UTIs.
•Haematuria.
•Bladder pain.
•Suspected urinary tract injury or fistula.
•To exclude bladder tumour or stones.
•If interstitial cystitis is suspected.

ASSESSMENT OF THE LOWER URINARY TRACT: IMAGING 659
Assessment of the lower urinary tract: imaging
Imaging of the lower urinary tract is not justified as a routine investigation in all women presenting with urinary symptoms, but should instead be targeted at specific indications.
•Ultrasonography: is widely used to:
•exclude incomplete bladder emptying
•check for congenital abnormalities, calculi, tumours
•detect cortical scarring of the kidneys.
•Plain abdominal radiograph: is useful for screening for a variety of conditions, including foreign bodies and calculi.
•Contrast-enhanced CT: is the imaging modality of choice for detecting and characterizing renal masses and renal tract calculi, as well as ureteric or bladder lesions.
•IV urography: can be used in women with neuropathic bladder or suspected congenital and acquired abnormalities, e.g. uterovaginal fistulae. However, contrast-enhanced CT would provide more accurate and rapid detection.
•Micturating cystourethrography: is useful to demonstrate bladder and urethral fistulae, vesicouretheric reflux, and anatomical abnormalities of the lower urinary tract, such as urethral diverticulae.
•MRI: remains predominantly a research investigative technique for incontinence and prolapse, because of its cost and availability. It is mainly used for characterization of renal or pelvic masses and tumour staging.
Conditions requiring imaging of urinary tract
•Recurrent UTIs.
•Haematuria.
•Urethral diverticula, which need to be differentiated from paravaginal cysts.
•Suspected ureteric injuries.
•Suspected urethral or vesical fistulae.
•Suspected malignancy or renal stones.

660 CHAPTER 22 Urogynaecology
Assessment of the lower urinary tract: urodynamic investigations
Urodynamics
‘Urodynamics’ describes a combination of tests that look at the ability of the bladder to store and void urine. The tests include uroflowmetry, post-void residual measurement, and cystometry. In addition, urethral pressure profilometry and video-urodynamic investigations may be undertaken.
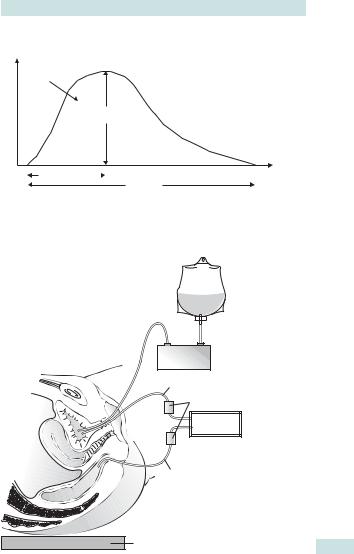
Uroflowmetry
Simple, non-invasive investigation that can be used to screen for voiding difficulties. The patient voids in privacy on a commode incorporating a urinary flow meter, measures voided volume over time, and plots it on a graph (Fig. 22.2).
Cystometry
•Involves measuring the pressure/volume relationship of the bladder during filling and voiding and is a useful test of bladder function.
•The bladder is filled with saline via a catheter, and the first sensation of filling, first desire to void, and any strong desire to void are recorded (Fig. 22.3).
•Electronic subtraction of the intra-abdominal pressure from the intravesical enables the detrusor pressure to be calculated (Fig. 22.4).
•During filling the patient is asked to cough at regular intervals and to stand, in order to provoke the bladder.
•The presence of detrusor contractions and leakage through the urethra are noted.
•The woman is then asked to void at the end of the test, for pressure/ flow analysis.
Video-urodynamics
•Combines fluoroscopic imaging of the bladder neck with cystometry, while filling the bladder with an iodine-based contrast medium.
•Enables detection of detrusor-sphincter dyssynergia, vesico-ureteric reflux, or presence of abnormalities in the renal tract that are commonly seen in women with neurogenic bladder problems.
Ambulatory urodynamic monitoring
•A small recording device is worn and the information is later downloaded to a computer for analysis and review.
•The bladder is filled naturally and the woman should carry out her normal daily activities, including those that provoke symptoms.
•This approach is particularly useful for investigating detrusor overactivity when standard laboratory urodynamics have failed to replicate
the symptoms experienced by the woman in her normal environment.
ASSESSMENT OF THE LOWER URINARY TRACT: URODYNAMICS 661
Flow rate (mI/s)
Volume
Maximum
flow rate
Time to maximum |
|
Time (s) |
|
Flow time
Fig. 22.2 Diagrammatic representation of normal urinary flow rate. Voided volume: total volume expelled via the urethra, the area beneath the flow-time curve. Maximum flow rate: maximum measured value of the flow rate. Average flow rate: volume voided divided by the flow time. Flow time: the time over which measurable flow actually occurs.
Peristaltic
pump
Intravesical pressure (Pves)
Pressure transducers
Computer
Intra-abdominal pressure (Pabd)
Tilting table
Fig. 22.3 Schematic drawing showing catheter positions during cystometry.
Three catheters are required: the first in the bladder to fill it; the second in the bladder to measure vesical pressure; and the third in the rectum to measure abdominal pressure. Reproduced with permission from Cardozo L, Staskin D (2001). Textbook of female urology and urogynaecology, published by Taylor and Francis, London.

STRESS URINARY INCONTINENCE: OVERVIEW 663
Stress urinary incontinence: overview
Definitions
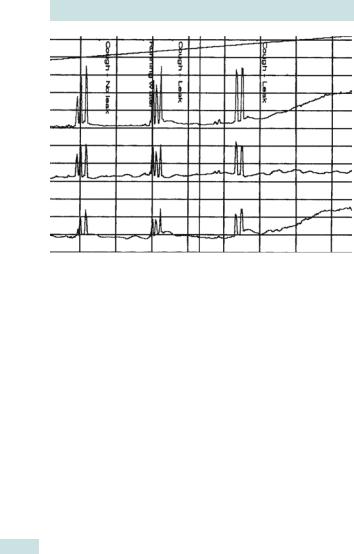
•Stress urinary incontinence (SUI): is the complaint of involuntary leakage of urine on effort or exertion, or on sneezing or coughing.
•Urodynamic stress incontinence (USI): is the involuntary leakage of urine during increased intra-abdominal pressure in the absence of detrusor contractions. Unlike SUI, it can only be diagnosed by urodynamic testing (Fig. 22.4).
Incidence
•The commonest urinary complaint for which women seek advice.
•1 in 10 women will suffer from it at some point in their lives.
•50% of incontinent women complain of pure stress incontinence.
•30–40% of incontinent women have mixed symptoms of urge and stress incontinence.
Pathophysiology and aetiology
•SUI occurs when the intravesical pressure exceeds the closing pressure on the urethra.
•Childbirth is the most common causative factor, leading to denervation of the pelvic floor, usually during delivery.
•Oestrogen deficiency at the time of menopause leads to weakening of the pelvic support and thinning of the urothelium.
•Occasionally, weakness of the bladder neck can occur congenitally, or through trauma from radical pelvic surgery or irradiation.
Clinical features
•Symptoms: typically a woman will complain of leakage of urine when she coughs, sneezes, runs, jumps, or carries heavy loads. The leakage is usually a small, discrete amount, coinciding with the physical activity.
•Signs: prolapse of the urethra and anterior vaginal wall may be present. It may be possible to demonstrate stress incontinence by asking the woman to cough with a fairly full bladder.
Investigations
•MSU sample: should be taken to exclude infection or glycosuria.
•Frequency/volume chart:
•typically shows normal frequency and functional bladder capacity
•slightly idiurnal frequency may be observed, as women may void more frequently to prevent leakage.
•Urodynamic studies should be considered when surgery is indicated to:
•confirm the diagnosis
•check for any co-existing detrusor overactivity
•check for voiding dysfunction.

664 CHAPTER 22 Urogynaecology
Stress urinary incontinence: conservative management
SUI interferes with a woman’s quality of life, but is not a life-threatening condition and therefore conservative measures should always be tried first. They include:
•Lifestyle interventions: weight reduction if BMI >30, smoking cessation, treatment of chronic cough and constipation.
•Pelvic floor muscle training: for at least 3mths should be considered as the first-line treatment:
•physiotherapists usually individualize the programme, but 3 sets of 8–12 slow maximal contractions sustained for 6–8s each per day is a common regimen
•the exercises need to be continued long term.
•Biofeedback: refers to the use of a device to convert the effect of pelvic floor contraction into a visual or auditory signal to allow women objective assessment of improvement.
•Electrical stimulation: can assist in production of muscle contractions in women who are unable to produce muscle contraction.
•Vaginal cones: have been developed as a way of applying graded resistance against which the pelvic floor muscles contract.
Pharmacological management of SUI
Duloxetine: is the only drug licensed for the treatment of moderate to severe SUI.
•It is an SNRI that enhances urethral striated sphincter activity via a centrally mediated pathway.
•However, it is of mediocre efficacy and is associated with significant side effects. It is not recommended for first-line use by NICE.
•Nausea is the most frequently reported side effect (up to 25%).
•Other side effects include dyspepsia, dry mouth, insomnia or drowsiness, and dizziness.
Indications for conservative treatment of stress urinary incontinence
•Mild or easily manageable symptoms.
•Family incomplete.
•Symptoms manifest during pregnancy.
•Surgery contraindicated by co-existing medical conditions.
•Surgery declined by patient.
This page intentionally left blank

668 CHAPTER 22 Urogynaecology
Overactive bladder syndrome: overview
Definition
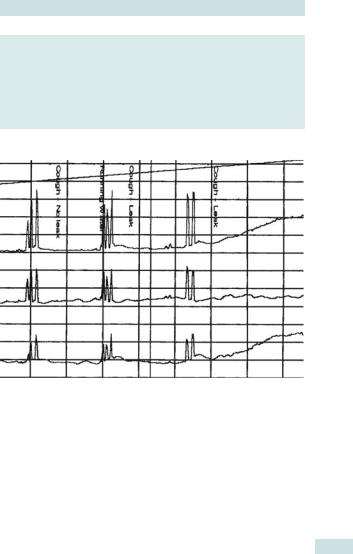
•OAB is a chronic condition, defined as urgency, with or without urge incontinence, usually with frequency or nocturia.
•It is used to imply probably underlying detrusor overactivity (DO), but this is a diagnosis made on urodynamic testing (Fig. 22.6).
Aetiology
•Idiopathic in most cases.
•Neurogenic DO is found in the presence of conditions such as multiple sclerosis, spina bifida, and upper motor neuron lesions.
•sto pelvic or incontinence surgery.
•OAB due to outflow obstruction is uncommon in women.
Clinical features of OAB
•Symptoms of OAB include urinary frequency, urgency, urge incontinence, and nocturia.
•Provocative factors often trigger it, such as cold weather, opening the front door, or hearing running water.
•Bladder contractions may also be provoked by iintra-abdominal pressure (coughing or sneezing), leading to complaint of stress incontinence, which may be misleading.
•Quality of life can be significantly impaired by the unpredictability and large volume of leakage.
Investigations
Urine culture
Exclusion of infection is mandatory, as symptoms overlap those of UTI.
Frequency/volume chart
•Typical features are idiurnal frequency associated with urgency and episodes of urge incontinence.
•Nocturia is a common feature of OAB.
Urodynamics
•Characterized by involuntary detrusor contractions during the filling phase of the micturition cycle, which may be spontaneous or provoked.
•Video-urodynamic testing is more appropriate in women with neurological diseases, to exclude vesicoureteric reflux or renal damage secondary to a persistent significant rise in intravesical pressure.
Diagnosis
•Urodynamic assessment is essential for the diagnosis of OAB in women with multiple and complex symptoms.
•Other factors, such as metabolic abnormalities (diabetes or hypercalcaemia), physical causes (prolapse or faecal impaction), or urinary pathology (UTI or interstitial cystitis), need to be excluded before the diagnosis of OAB is made.
OVERACTIVE BLADDER SYNDROME: OVERVIEW 669
Key points
•OAB is a common condition affecting around 1 in 6 women.
•The incidence of OAB increases with age.
•OAB is the second most common cause of urinary incontinence.
•OAB is the most common cause of incontinence in older women.
•Urodynamic assessment is required to make a diagnosis of DO.
•QoL is often severely affected by OAB symptoms.
Fig. 22.6 Urodynamic trace showing detrusor overactivity. The upper trace of intravesical pressure (Pves) vs. time shows a sharp increase of pressure within the bladder. The middle trace of pressure within the abdomen (Pabd) shows no similar increase. The lower trace, obtained by subtracting intra-abdominal pressure from intravesical pressure (Pdet = Pves – Pabd), shows significant detrusor overactivity.

670 CHAPTER 22 Urogynaecology
Overactive bladder syndrome: management
Conservative management
It is wise to start with the simplest of conservative therapies and progress through to more radical treatments if necessary.
Behavioural therapy
•Advice to consume 1–1.5L of liquids per day.
•Avoid caffeine-based drinks (tea, coffee, cola) and alcohol.
•Various drugs, such as diuretics and antipsychotics, alter bladder function and should be reviewed.
Bladder retraining
•The principles of bladder retraining are based on the ability to suppress urinary urge and extend the intervals between voidings.
•Reported cure rates using bladder retraining alone are 44–90%.
Hypnotherapy and acupuncture
•These can be successful in some cases.
•The relapse rate is very high.
Pharmacological interventions
Anticholinergic (antimuscarinic) drugs
•These remain the mainstay of pharmacotherapy; they block the parasympathetic nerves, thereby relaxing the detrusor muscle.
•Patients should be advised about the side effects before starting treatment (some preparations may be better tolerated than others) (Table 22.2).
•The dosage may need to be titrated against efficacy and adverse effects.
•Adverse effects of anticholinergics may include:
•dry mouth (up to 30%)
•constipation, nausea, dyspepsia, and flatulence
•blurred vision, dizziness, and insomnia
•palpitation and arrhythmias.
Contraindications to anticholinergics
•Acute (narrow angle) glaucoma.
•Myasthenia gravis.
•Urinary retention or outflow obstruction.
•Severe ulcerative colitis.
•Gastrointestinal obstruction.
Oestrogens
•Intravaginal oestrogens may be tried in women with vaginal atrophy.
•Treatment with vaginal oestrogen often helps with symptoms of urgency, urge incontinence, frequency, and nocturia.
OVERACTIVE BLADDER SYNDROME: MANAGEMENT 671
Use of botulinium toxin A for OAB
•Botulinium toxin A blocks neuromuscular transmission, causing temporary paralysis.
•Increasingly used as an intervention for refractory overactive bladder, with an efficacy of up to 90%.
•It is injected cystoscopically into the detrusor, usually under local anaesthetic.
•It can cause urinary retention in 5–10% of cases, in which case intermittent self-catheterization may be required.
•Repeat injections are required every 6–12mths.
•The long-term effects of repeat injections are unknown and are the subject of ongoing research.
Neuromodulation and sacral nerve stimulation
•Provides continuous stimulation of the S3 nerve root via an implanted electrical pulse generator and is thought to improve the ability to suppress detrusor contractions.
•It is being used increasingly in the treatment of refractory detrusor overactivity.
•Overall, neuromodulation has up to 50% clinical success rate.
Surgical management of OAB
•Surgery is reserved for those with debilitating symptoms and who have failed to benefit from medical, behavioural, and/or neuromodulation therapy.
•Procedures such as detrusor myomectomy and augmentation cystoplasty have limited efficacy and complication rates are high.
•Permanent urinary diversion is occasionally indicated in women with intractable incontinence.
Table 22.2 Anticholinergic drugs and their dosages
Drug |
Delivery route |
Adult dosage |
Selectivity |
|
|
Oxybutynin |
(a) Oral |
2.5–5mg, |
Selective, |
|
|
|
|
1–4 times/day |
predominantly M1 |
|
|
|
|
|
and M3 |
|
|
|
(b) Transdermal |
1 patch, twice weekly |
|
|
|
|
patch |
(3.9mg/24h) |
|
|
|
Propiverine |
Oral only |
15mg, 2–4 times/day |
Non-selective |
|
|
Solifenacin |
Oral only |
5–10mg daily |
Selective, |
|
|
|
|
|
predominantly M3 |
|
|
Tolterodine |
Oral only |
(a) 2mg, bd |
Non-selective |
|
|
|
|
(b) 4mg, od |
|
|
|
|
|
(sustained release) |
|
|
|
Trospium |
Oral only |
20mg, bd |
Non-selective |
|
|
Fesoterodine |
Oral only |
4 or 8mg, od |
Selective, |
|
|
|
|
(sustained release) |
predominantly M3 |
|
|
|
|
|
|
|
|

672 CHAPTER 22 Urogynaecology
Anatomy of the pelvic floor
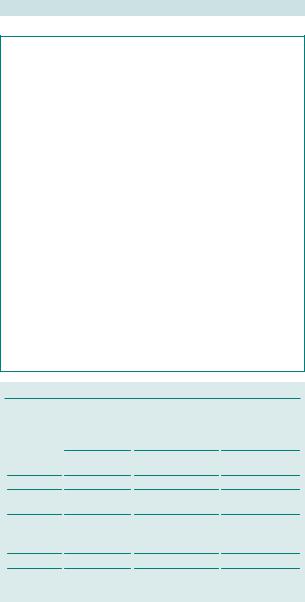
The pelvic floor consists of muscular and fascial structures that provide support to the pelvic viscera and the external openings of the vagina, urethra, and rectum (Fig. 22.7). The uterus and vagina are suspended from the pelvic side walls by endopelvic fascial attachments that support the vagina at three levels.
Three levels of vaginal support
•Level 1: the cervix and upper third of the vagina are supported by the cardinal (transverse cervical) and uterosacral ligaments. These are attached to the cervix and suspend the uterus from the pelvic sidewall and sacrum respectively.
•Level 2: the mid portion of the vagina is attached by endofascial condensation (endopelvic fascia) laterally to the pelvic side walls.
•Level 3: the lower third of the vagina is supported by the levator ani muscles and the perineal body. The levator ani, together with its associated fascia, is termed the pelvic diaphragm.
The axis of the vagina is also important. It normally lies in a horizontal plane, flat on the levator muscles. This protects it during coughing and other activities that increase intra-abdominal pressure (Fig. 22.7).
1 Damage occurring at the different levels of vaginal support causes different types of prolapse. It is therefore important to have an understanding of this anatomy.
Aetiology of prolapse
•Pregnancy and vaginal delivery: prolapse is uncommon in nulliparous women. Vaginal delivery may cause mechanical injuries and denervation of the pelvic floor. The risk is increased with large babies, prolonged second stage, and instrumental delivery (particularly forceps).
•Congenital factors: abnormal collagen metabolism, for example, in Ehlers–Danlos syndrome, can predispose to prolapse.
•Menopause: the incidence of prolapse increases with age. This may be due to the deterioration of collagenous connective tissue that occurs following oestrogen withdrawal.
•Chronic predisposing factors: prolapse is aggravated by any chronic increase in intra-abdominal pressure, resulting from factors such as obesity, chronic cough, constipation, heavy lifting, or pelvic mass.
•Iatrogenic factors: pelvic surgery may also influence the occurrence of prolapse:
•hysterectomy is associated with subsequent vaginal vault prolapse (particularly when the indication was prolapse)
•continence procedures, although elevating the bladder neck, may lead to defects in other pelvic compartments (Burch colposuspension may predispose to rectocele and enterocele formation).
ANATOMY OF THE PELVIC FLOOR 673
(a)
Round ligament
Cardinal ligament 
Pelvic brim 
Levator ani 
Ischiopubic ramus 
Perinea muscle 
(b) |
Uterosacral ligament |
|
Levator ani |
Pubic symphysis
Perineal body
Fig. 22.7 (a) Coronal view of the pelvis, showing cardinal ligaments and levator ani. (b) Lateral view of the pelvis, showing the uterosacral ligaments and levator ani. Reproduced with permission from Impey L. (1999). Obstetrics and Gynaecology. Oxford: Wiley-Blackwell Publishing.

676 CHAPTER 22 Urogynaecology
Prolapse: clinical assessment
Symptoms
Symptoms are often absent, but the most commonly reported are:
•General:
•dragging sensation, discomfort, and heaviness within the pelvis
•feeling of ‘a lump coming down’
•dyspareunia or difficulty in inserting tampons
•discomfort and backache.
•Cysto-urethrocele:
•urinary urgency and frequency
•incomplete bladder emptying
•urinary retention or reduced flow where the urethra is kinked by descent of the anterior vaginal wall.
•Rectocele:
•constipation
•difficulty with defecation (may digitally reduce it to defecate).
Symptoms tend to become worse with prolonged standing and towards the end of the day. In case of grade 3 or 4 prolapse, there may be mucosal ulceration and lichenification, resulting in vaginal bleeding and discharge.
Examination
•Exclude pelvic masses with a bimanual examination.
•Vaginal examination is best carried out with the woman in the left lateral position, using a Sims speculum.
•The walls should be checked in turn for descent and atrophy.
•If absolutely necessary, a volsellum may be applied to the cervix so that traction will demonstrate the severity of uterine prolapse (this can cause marked discomfort and should be performed very gently).
•Sometimes, prolapse may only be demonstrated with the woman standing or straining.
•An assessment of pelvic floor muscle strength should be carried out (see Box 22.1).
Quality of life assessment
•Symptoms can affect quality of life, causing social, psychological, occupational, or sexual limitations to a woman’s lifestyle.
•Self-completion questionnaires allow a comprehensive assessment of prolapse symptoms and their impact, such as the Vaginal Symptoms module of the International Consultation on Incontinence Questionnaire (ICIQ-VS) (Mwww.iciq.net).
Investigations
•USS to exclude pelvic or abdominal masses (if suspected clinically).
•Urodynamics are required if urinary incontinence is present.
•ECG, CXR, FBC, and U&E (if appropriate), to assess fitness for surgery.
PROLAPSE: CLINICAL ASSESSMENT 677
Box 22.1 Modified Oxford system for grading pelvic floor muscle strength
A system of grading using vaginal palpation of the pelvic floor muscles.
•0: No contraction.
•1: Flicker.
•2: Weak.
•3: Moderate.
•4: Good (with lift).
•5: Strong.
678 CHAPTER 22 Urogynaecology
Prolapse: conservative management
Prevention of pelvic organ prolapse
•Reduction of prolonged labour.
•Reduction of trauma caused by instrumental delivery.
•Encouraging persistence with postnatal pelvic floor exercises.
•Weight reduction.
•Treatment of chronic constipation.
•Treatment of chronic cough (including smoking cessation).
Physiotherapy
Physiotherapy has a role in the management of mild prolapse in younger women, who find intravaginal devices unacceptable and are not yet willing to consider definitive surgical treatment.
•Pelvic floor muscle exercises (PFME): are most effective when taught under the direct supervision of a physiotherapist; these will improve the tone in young parous women, but are unlikely to benefit older women with significant uterovaginal prolapse.
•Biofeedback and vaginal cones (see bStress urinary incontinence: conservative management, p. 664).
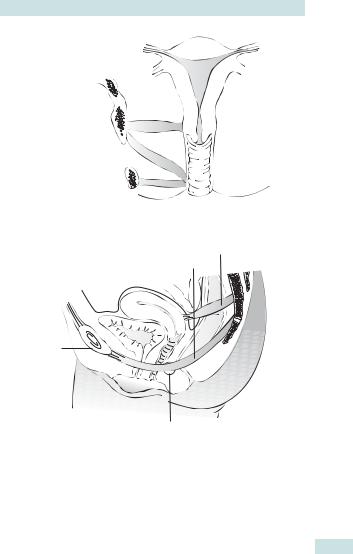
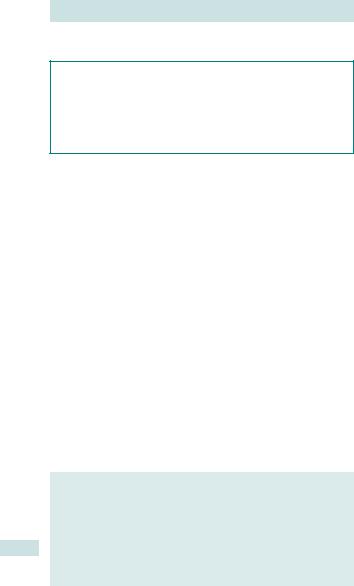
Intravaginal devices (pessaries)
Vaginal pessaries (Fig. 22.9) offer a further conservative line of therapy for women who decline surgery, who are unfit for surgery, or for whom surgery is contraindicated. They should be changed 6 monthly and topical oestrogen may be given to reduce the risk of vaginal erosion.
•Ring pessary: is most commonly used and is available in a number of different sizes (52–129mm); the ring is placed between the posterior aspect of the symphysis pubis and the posterior fornix of the vagina.
•Shelf pessary: can be used when a correctly sized ring pessary will not sit in the vagina and/or where the perineum is deficient (it may be difficult to insert and remove, so its use is becoming less common).
•Hodge pessary: can be used to correct uterine retroversion. It is of classical interest, but in practice is virtually never used now.
•Cube and doughnut pessaries: are, very rarely, used for significant prolapse, when others are not retained.
Factors influencing management of prolapse
•Severity of symptoms.
•Extension of the signs (asymptomatic grade 1 prolapse does not require treatment).
•Age, parity, and wish for further pregnancies.
•Patient’s sexual activity.
•Presence of aggravating features such as smoking and obesity.
•Urinary symptoms.
•Other gynaecological problems such as menorrhagia.
PROLAPSE: CONSERVATIVE MANAGEMENT 679
Fig. 22.9 Types of pessary for uterine prolapse include rings, cubes, shelf, and doughnuts. Reproduced by courtesy of Milex Products Inc., Chicago © 2002

This page intentionally left blank

682 CHAPTER 22 Urogynaecology
Prolapse: surgical management, uterovaginal and vault
Uterovaginal (apical) prolapse
Vaginal hysterectomy
May be combined with the above procedures, in cases of significant uterine descent or menstrual problems (Table 22.3).
Manchester repair (or Fothergill repair)
•Now rarely performed.
•Cervical amputation is followed by approximation and shortening of the cardinal ligaments anterior to the cervical stump.
•This is combined with an anterior and posterior colporrhaphy.
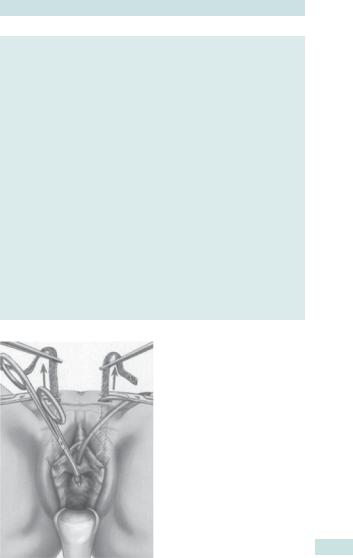
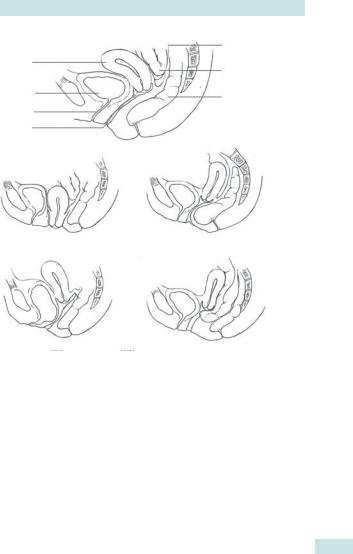
Hysteropexy
•Can be performed if patient wishes to preserve uterus as an open or laparoscopic procedure (Fig. 22.10).
•Uterus and cervix are attached to sacrum using bifurcated non-absorbable mesh.
•Theoretical advantage of hysteropexy is stronger apical support when compared with vaginal hysterectomy.
Vaginal vault prolapse
Sacrospinous ligament fixation
•Involves suturing the vaginal vault to the sacrospinous ligaments, using a vaginal approach.
•Low immediate postoperative morbidity; success rate 70–85%.
1As vaginal axis is changed by this procedure, there is risk of postoperative dyspareunia.
Sacrocolpoplexy
•The vault is attached to the sacrum using a non-absorbable mesh, and if can be performed either as an open procedure or laparoscopically.
•It has a higher success rate, of around 90%, and a better anatomical result than sacrospinous fixation.
1 Mesh erosion into the vagina, or rarely into the bladder or bowel, is a possible late complication.
Recurrent urogenital prolapse
•Approximately 1/3 of all prolapse surgery is for recurrent defects.
•Vaginal epithelium may be scarred and atrophic:
•making surgical correction technically more difficult
•increasing the risk of damage to the bladder and bowel.
•Use of synthetic meshes is becoming increasingly common for repair of recurrent prolapse, as they may offer more support where endopelvic fascia has proved to be deficient.
PROLAPSE: SURGICAL MANAGEMENT, UTEROVAGINAL AND VAULT 683
Table 22.3 Operations available for uterovaginal prolapse
Defect |
Vaginal route |
Abdominal route (open or |
|
|
laparoscoic) |
|
|
|
Anterior |
Anterior colporrhaphy |
Paravaginal repair; sacrocolpopexy |
|
Transvaginal mesh repair |
with placement of the mesh over |
|
anterior vaginal wall |
|
|
|
|
Apical |
Vaginal hysterectomy; |
Hysteropexy (laparoscopic or |
|
sacrospinous fixation |
open); sacrocolpopexy |
Posterior |
Posterior repair; transvaginal |
Sacrocolpopexy to correct recto/ |
|
mesh repair; perineal body |
enterocele |
|
reconstruction |
|
|
|
|
Fig. 22.10 Bifurcated mesh in position for sacrohysteropexy. Reproduced from Springer-Verlag London Ltd., Female Pelvic Reconstructive Surgery, 2002, p 187, Figure 13.10 Stanton and Zimmern. With kind permission of Springer Science and Business Media.
This page intentionally left blank