

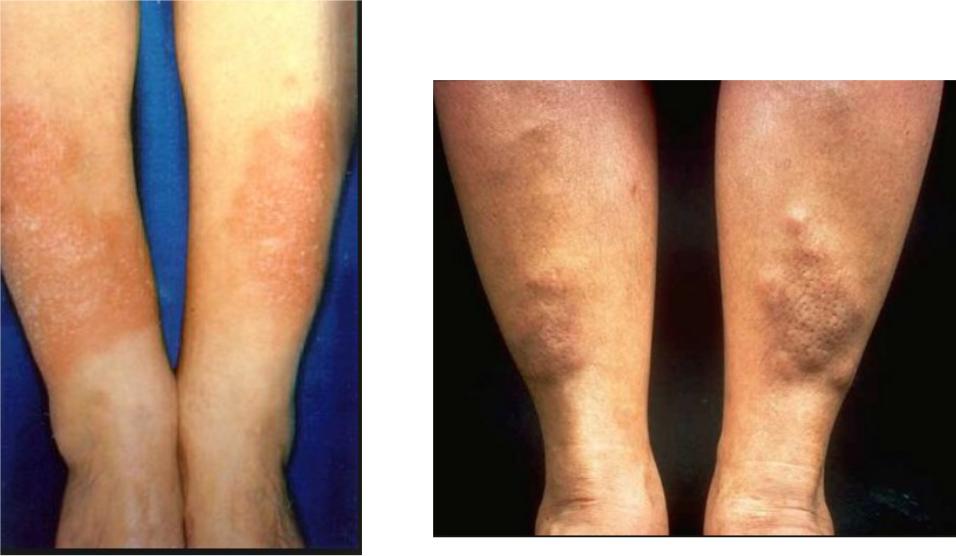
Pretibial myxedema
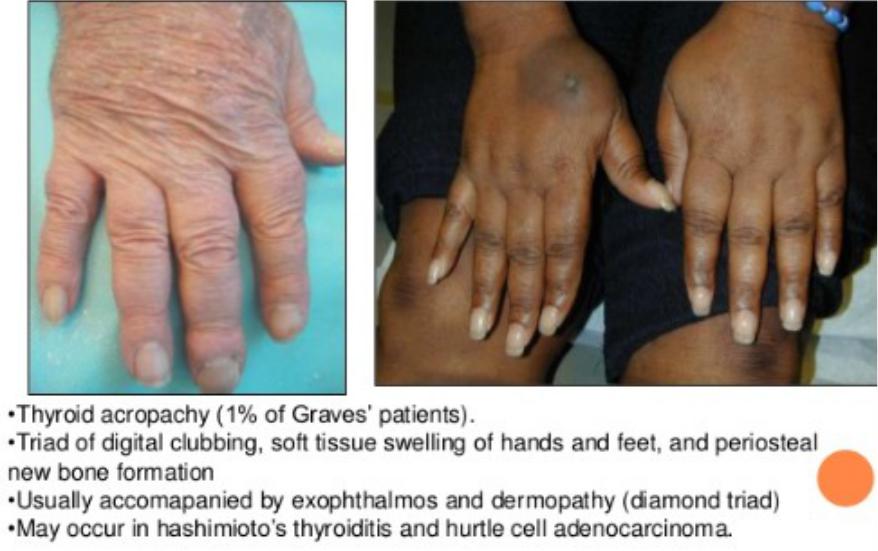
Thyroid acropathy
Difference in thyrotoxicosis presentation
•Younger patients tend to exhibit symptoms of sympathetic activation (eg, anxiety, hyperactivity, tremor)
•Older patients have more cardiovascular symptoms (eg, dyspnea, atrial fibrillation) and unexplained weight loss
•Patients with Graves disease often have more marked symptoms than patients with thyrotoxicosis from other causes
•Ophthalmopathy (eg, periorbital edema, diplopia, or proptosis) suggests Graves disease
Diagnostic evaluation in thyrotoxicosis
Laboratory tests
•Low TSH
•High T3 and T4
•Patients with milder thyrotoxicosis may have elevation of T3 levels only
•Subclinical hyperthyroidism presents with decreased TSH and normal T3 and T4levels
•Anemia, elevated ESR
•Low TC and TG
•High ALT, AST, AP
•Hyperglycemia
Instrumental methods
•Thyroid ultrasound:
–Diffuse enlargement
–Increased blood flow
–Nodules
•Scintigraphy
–Diffuse uptake increase
–Hot nodules
•Aspiration biopsy
Autoantibody tests for hyperthyroidism
•Anti–thyroid peroxidase (anti-TPO) antibody - Nonspecific elevation with autoimmune thyroid disease found in 8% of Graves patients
•Thyroid-stimulating antibody (TSab) - Also known as thyroid-stimulating immunoglobulin (TSI), long-acting thyroid stimulator (LATS), or TSH-receptor antibody (TRab); found in 63-81% of Graves disease; a positive test is diagnostic and specific for Graves disease
Autoantibody titers in hyperthyroidism
•Graves disease - Significantly elevated anti-TPO, elevated TSab
•Toxic multinodular goiter - Low or absent anti-TPO and TSab
•Toxic adenoma - Low or absent anti-TPO and TSab
•Patients without active thyroid disease may have mildly positive anti-TPO and TSab

Scintigraphy in thyrotoxicosis
The degree and pattern of isotope uptake indicates the type of thyroid disorder
•Graves disease – Diffuse enlargement of both thyroid lobes, with uniform uptake of isotope and elevated radioactive iodine uptake
•Toxic multinodular goiter -- Irregular areas of relatively diminished and occasionally increased uptake; overall radioactive iodine uptake is mildly to moderately increased
•Subacute thyroiditis –Very low radioactive iodine uptake
Grave`s disease
•The most common cause of endogenous hyperthyroidism
•Prevalence 1%
•Peak incidence in women 20-40 years old
•Etiology:
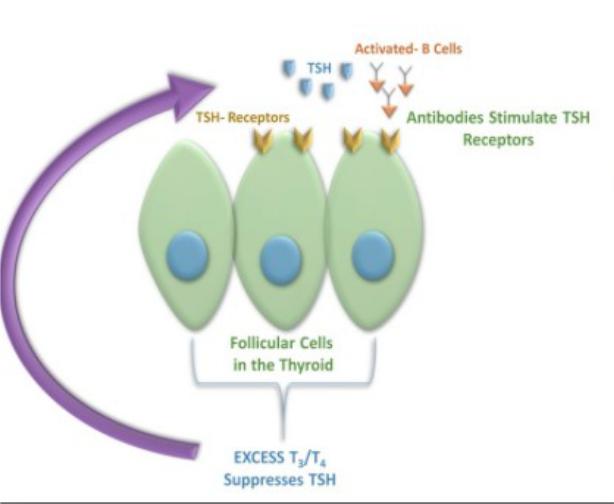
•Autoimmune
•Associated with other autoimmune diseases
•Stimulating immunoglobulins
•Hereditary
•Infections
•Trauma
Clinical presentation of Grave`s disease
•Thyrotoxicosis
•Diffuse goiter
•Ophtalmopathy
•Dermopathy
•Lymphadenopathy, splenomegaly, enlargement of the thymus
•High incidence of other autoimmune diseases
