


Alcohol-induced hepatic lesions
• only a minority of consistently heavy drinkers with hepatic steatosis (15 to 20 %) ever have clinically important liver disease (LD)
•Risk factors for serious liver damage in habitual alcohol drinkers include certain polymorphisms in alcohol- metabolizing enzymes, obesity, exposure to other hepatotoxins (e.g., acetaminophen), and infection with hepatitis C
•In many patients, a specific RF is never identified.

Pathogenesis of liver injury secondary to chronic ethanol ingestion
•MAA, malondialdehyde-acetaldehyde
•TNF-a, tumor necrosis factor a
•TGF-b, transforming growth factor b; IL, interleukin

Equivalents of pure alcohol
• |
Strong drinks |
28 ml |
10 g |
• |
Vine |
85 ml |
10 g |
• |
Beer |
230 ml |
10 g |
• |
Minimal dose |
|
|
that cause liver damage - 30 g/day
• 210 g ethanol per week is safe ?

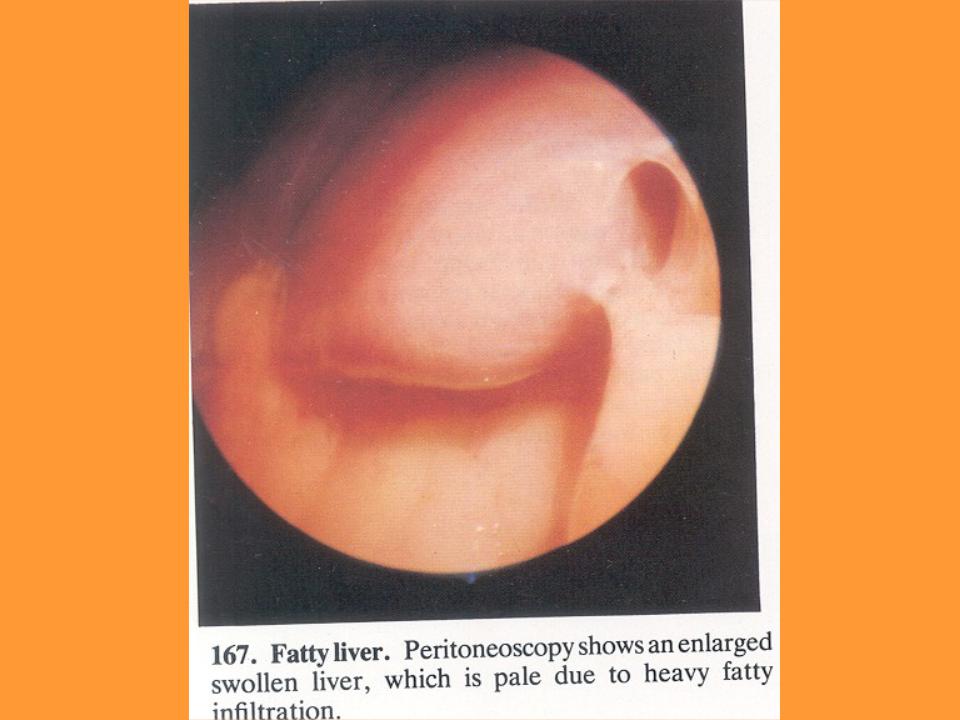
Alcoholic fatty liver
•Clinical manifestations are often minimal or entirely absent
•the disorder may not be recognized unless another illness (frequently alcohol-related) brings the patient to medical attention
•Hepatomegaly, at times accompanied by tenderness, may be the only finding
•Jaundice, ascites, and edema are seen only with more serious liver injury.

Two-Hit Model of the Progression of Fatty Liver Disease
•The earliest stages of FLD involve exposure of hepatocytes to TNF-a
•TNF-a initiates various intracellular signals mitochondrial permeability and the release of reactive oxygen species (ROS).
•Left unchecked, these responses promote hepatocyte apoptosis.
•Most healthy hepatocytes use some of the potentially lethal signals (e.g.,ROS) to activate a multifaceted response that permits
the hepatocytes to survive.
•Secondary insults (second hits) that inhibit this adaptation also result in apoptosis
•Even when adaptation is successful and hepatocytes remain viable, they become extremely vulnerable to other insults that partially depolarize the mitochondrial inner membrane, dying by necrosis when the mitochondrial membrane potential collapses.

Alcoholic fatty liver
•Fatty liver invariably develops after heavy alcohol intake
•It can progress to alcoholic hepatitis and cirrhosis
•In some patients, alcoholic hepatitis is a necessary step in the development of alcohol-induced cirrhosis
•However, in some other patients alcohol may stimulate the production of fibrosis and cirrhosis without requiring alcoholic hepatitis as an intermediate lesion.

Similarities between Alcoholic and Nonalcoholic Fatty Liver Diseases
• |
Obesity (OB) and alcohol abuse (AA) are associated with the |
same |
spectrum of |
|
liver diseases. |
|
|
|
|
• |
The time course for the progression of disease and the RR of |
cirrhosis are also |
||
similar in obesity-related liver disease |
(ORLD)and ARLD |
|
|
|
• |
Distinct, but mutually enhancing, mechanisms may also be |
involved |
|
|
• |
The similar pathologic features and natural histories of the two |
types of |
||
FLD suggest that common pathogenic mechanisms may be involved. |
|
|||
• |
A fatty liver is more common in pts with OB and AA than in those with either |
|||
alone. |
|
|
|
|
• |
Moreover, OB is an independent RF for cirrhosis in pts who AA Thus, elucidation |
|||
of the mechanisms that cause ORLD is |
liikely to clarify the role of pluripotent |
|||
cytokines, such as TNF- a , in promoting alcohol-induced liver damage.

Alcoholic hepatitis
• The clinical features AH resemble those of viral or toxic liver injury
–anorexia, nausea and vomiting, malaise, weight loss, abdominal distress, and jaundice
–Fever is seen in about half of cases.
•On physical examination
–tender hepatomegaly is common
–splenomegaly is found in about one-third of patients
–the patient may have cutaneous arterial "spider" angiomas and jaundice
More severe cases may be complicated by ascites, edema, bleeding, and encephalopathy.
This figure depicts a laparoscopic view of a patient with chronic active hepatitis and early cirrhosis
