

6 курс / Кардиология / И_А_Овсыщер_Реальна_ли_профилактика_ФП
.pdfРеальна ли профилактика ФП?
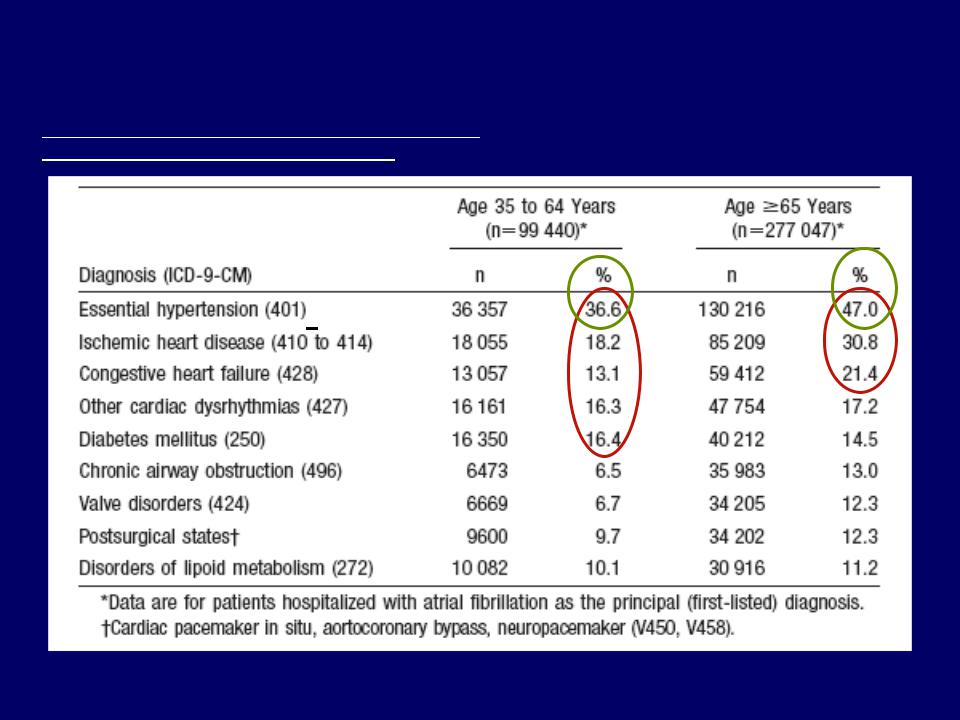
Comorbidities Among Adults >35 Years of Age Hospitalized in 1999 with AF: National (US) Hospital Discharge Survey
From Wattigney, et al. Circulation. 2003;108:711-716. Khairallah et al. Am J Cardiol 2004;94:500.
*
*АГ и ФП в РФ

Реальна ли профилактика ФП?
*Upstream or Non-Anti-arrhythmic Therapy
β-blockers
ACEI
ARB
Statins
PUFAs
*Non-traditional
Contrary to popular opinion and customs

Non-anti-arrhythmic Drugs or Upstream Therapy to Prevent AF
There is accumulating evidence in support of the antiarrhythmic effects of non-anti-arrhythmic drugs such as:
Angiotensin-converting enzyme inhibitors (ACEI)
Angiotensin-receptor blockers (ARB)
Anti-inflammatory agents
Statins
Omega-3 fatty acids (N-3 polyunsaturated fatty acidsPUFAs).
Effect of the non-anti-arrhythmic drugs seem promising, over and above any effect related to the treatment of underlying disease.

Angiotensin-converting enzyme inhibitors (ACEI) & Angiotensin-receptor blockers (ARB) to prevent AF
After Dorian P, et al. Eur Heart J 2008;Supll H, 11-31
Multiple effect of ACEIs and ARBs:
Anti-inflammatory, anti-oxidant, anti-fibrotic effects,
Prevention LA stretch/dilation & atrial remodeling attenuation
Regression LVH
Autonomic nervous system regulation
Modulation ion-channel function; can modify gap junction properties to prevent worsening of cell communication in cardiomyopathy.

Angiotensin-converting enzyme inhibitors (ACEI) & Angiotensin-receptor blockers (ARB) to prevent AF
The Guidelines of ESC for the management Arterial Hypertension and Guidelines of ACC/AHA/ESC for the management of AF indicate that ACEI/ARB may be preferable for both 10 & 20 prevention of AF associated with hypertension, MI, HF, or DM

Registered ACEI/ARB Clinical Trials (14)
CTAF-2 - A prospective, randomized, double-blind placebo-controlled study with 8 mg/d oral perindopril to prevent the recurrence of AF in pts with hypertension
DRAFT -the use of DIOVAN to reduce post-cardioversion recurrence of AF, randomized, double-blind, placebo controlled study
Trial to Investigate the Efficacy of Olmesartan in PAF
GISSI-AF- use of Valsartan an ARB in the Prevention of AF Recurrence - randomized, double blind, placebo controlled study. NEJM 2009.
ACTIVE-Substudy evaluating the effects of irbesartan on recurrences of PAF
ONTARGET/TRANSCEND (AF: secondary endpoint)-randomized, double-blind,
A randomized clinical trial of prevention of p/ablation recurrence of AF with valsartan-randomized, double-bllind, placebo control
A retrospective analysis of the use of ACEIs and ARBs on post-operative AF
Irbesartan for the prevention of atrial arrhythmias & cardiac electrical remodeling in pts with hypertension, pacemakers and risk factors for developing AF
Impact of Irbesartan on oxidative stress and C-reactive protein levels in pts with persistent AF - randomized, double-blind, placebo control
RAAS, inflammation, and post-operative AF - randomized, double-blind, placebo control
LV reverse remodeling after aortic valve replacement in severe AS-effect of blockade of ARB-randomized, open label, active control
Comparison of two treatments to decrease inflammation and AF following cardiopulmonary bypass surgery.
Electrophysiological effects of irbesartan in pts with PAF-randomized, doubleblind, placebo control.

Anti-inflammatory Agents
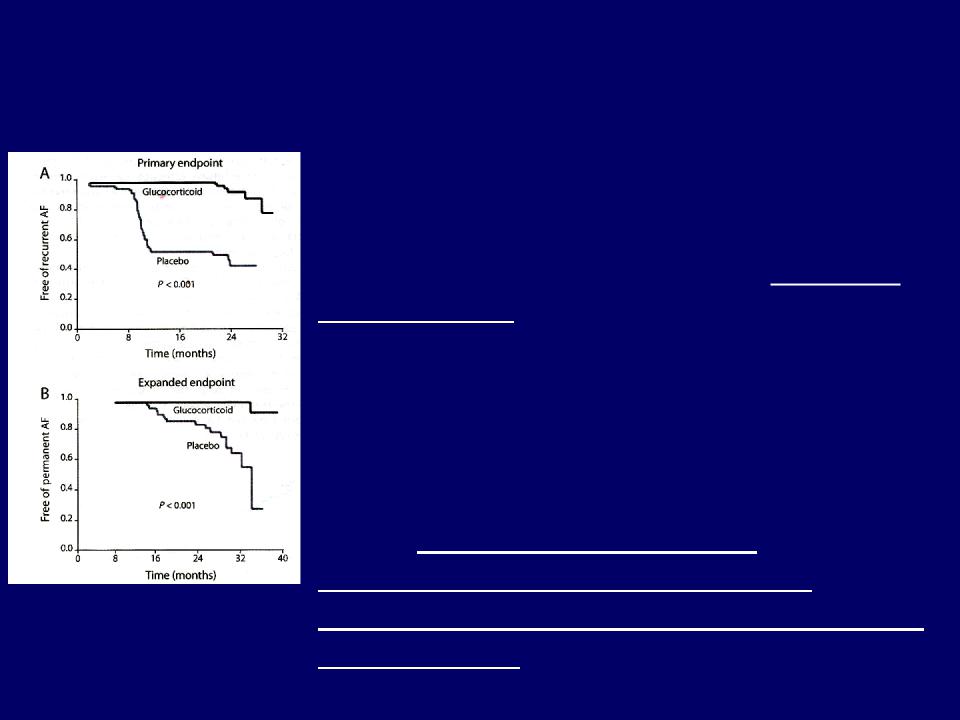
Main results of a study of Prednisolone to prevent recurrence of permanent AF in pts successfully
converted to SR
A double-blind study of 104 pts with normal LV function and persistent AF converted to SR by amiodarone or DC cardioversion. 59 pts were randomized to receive low-dose Prednisolone or placebo. Propafenone (450 mg/d) was administered to all pts and was maintained during the entire FU period (median: 23 mo). Compared with placebo, Prednisolone reduced recurrent AF from 50% to 9.6% and permanent AF from 29% to 2%. Survival distributions for Prednisolone and for placebo were significantly different for both recurrent and permanent AF (P < 0.001).

Statins and AF
Results of 16 animal & clinical studies. Adapted after Kostapanos et al. Cardiovasc. Res 2007;75:10-20. Savelieva I, Camm J. Nat Clin Pract Cardiovasc Med 2008;5:30–41.
Statins have shown multiple beneficial effects beyond lowering of cholesterol:
Anti-inflammatory, anti-oxidant, anti-fibrotic effects
May be able to decelerate or even reverse atrial structural remodeling in patients with AF
Protecting atrial myocardium during ischemia
Improves coagulation function-decreases risk of stroke
Autonomic nervous system regulation.
In the Guidelines of ACC/AHA/ESC for the management of AF stated: the use of statins may protect against AF, however this use is still insufficiently explored.