

4 курс / Дерматовенерология / Дерматоскопия (3)
.pdf© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
90 Pattern Analysis – Basic Principles
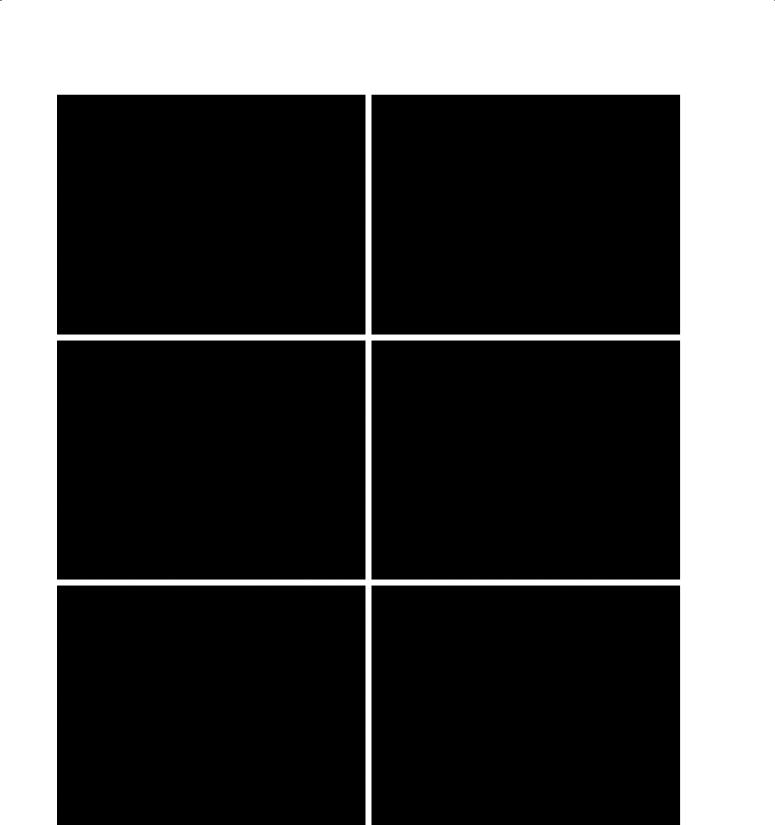
Figure 3.48: Labial lentigines.
Top row: labial lentigo with the structureless pattern. Middle and bottom rows: labial lentigines with two dermatoscopic patterns, brown curved lines and circles.
Genital lentigo, Labial lentigo
Pattern |
Colors |
Clues |
1. Structureless |
Typical: |
None |
2. Parallel lines, curved |
Light-brown to dark-brown, rarely with |
|
3. Circles |
gray or black |
|

© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
Pattern Analysis – Basic Principles |
91 |
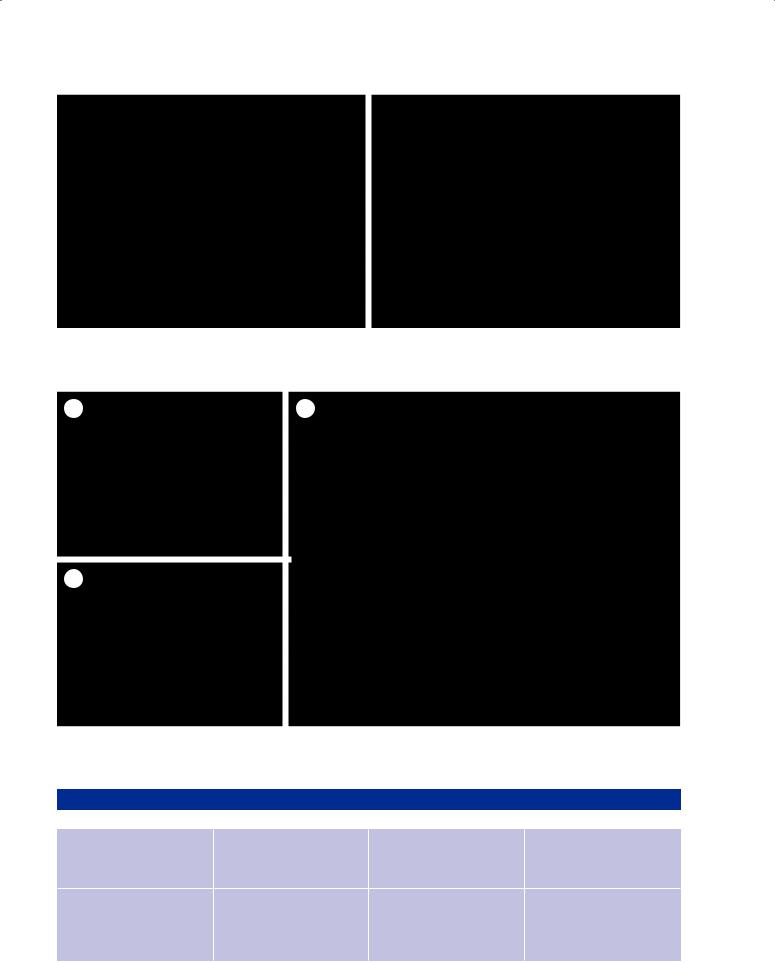
Figure 3.49: Pigmented basal cell carcinomas. Dermatoscopy in right column.
Top row: The pattern is a combination of radial lines at the periphery (white arrow) and a large structureless zone. Clues include a few blue clods (black arrow) and red clods as a sign of ulceration with hemorrhage. Second row: Two patterns, structureless (skin-colored) and clods, some of which are blue and gray. The vessels are serpentine but not branched (the definition of branched requires that the vessel of origin be thicker than the branches). Third row: In this basal cell carcinoma the clod pattern is predominant. These clods vary in size and shape, and are predominantly blue, with only a few being brown. The vessels are serpentine, with some branched. Bottom row: A typical pattern of pigmented basal cell carcinoma; clods which are blue, grey and brown.
© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
92 Pattern Analysis – Basic Principles
Figure 3.50: Pigmented basal cell carcinoma.
Top row: This typical basal cell carcinoma on the trunk has two patterns on dermatoscopy, structureless and radial lines, combined asymmetrically. Clues to the diagnosis of basal cell carcinoma are: gray dots, the radial lines converge to a common base, a few blue clods (at 9 o’clock position) and central serpentine vessels. Middle row: Two patterns, structureless and dots, arranged asymmetrically, and serpentine vessels, yield the diagnosis of a basal cell carcinoma. Bottom row: One pattern: blue clods, and serpentine branched vessels, are typical characteristics of a pigmented basal cell carcinoma.

© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
|
Pattern Analysis – Basic Principles |
93 |
||
|
|
|
|
|
Pigmented basal cell carcinoma |
|
|
|
|
Pattern |
Colors |
Clues |
|
|
Typical: |
Typical: |
Typical: |
|
|
1. Clods of different sizes and shapes |
Clods = blue, gray, or brown |
1. Peripheral radial lines with a common base |
||
2. Peripheral radial lines (occasionally) |
Dots = gray or blue, occasionally brown |
2. |
Radial lines that converge at a central dot |
|
3. Dots |
Structureless area = skin-colored, white or |
|
or clod |
|
4. Structureless |
orange |
3. |
Blue or gray clods |
|
The pattern of clods and structureless may |
Radial lines = brown |
4. Orange structureless area |
|
|
occur alone or in combination with other |
|
5. |
Blue or gray dots |
|
patterns. Radial lines, on the other hand, |
|
6. |
Central structureless area, white or |
|
occur in basal cell carcinoma only in com- |
|
|
skin-colored |
|
bination with other patterns. |
|
7. Branched vessels or thin serpentine vessels |
||
Pigmented Bowen’s disease
Pigmented Bowen’s disease shows two common patterns. The most common is structureless and brown (3.52). Less common, but more specific is an asymmetric combination of brown and/or gray dots (or more rarely small brown clods), and a hypopigmented (pink, white, or skin colored) structureless area. Vessels are coiled and usually seen in hypopigmented zones (3.53). At 10x magnification these vessels may resolve as dots rather than coils. Arrangement of vessels may be linear, random or clustered. A few white clods may be seen, being a dermatoscopic sign of surface scale. The arrangement of brown and/or gray dots as radial lines is an important clue (3.53). Coiled vessels may also be incorporated into these radial lines.
Reticular lines should be absent, their presence being a strong clue to consider an alternative diagnosis. If they are present they usually indicate a collision with solar lentigo. For lesions on lighter skin phototypes, the presence of black pigmentation is also a clue against the diagnosis of pigmented Bowen’s disease. The derma-
toscopic presentation of pigmented Bowen’s disease is the same irrespective of whether it has been induced by UV radiation, chemicals such as arsenic, or, by human papilloma virus (HPV) infection as shown in figure 3.54.
Correlation between dermatoscopy and dermatopathology
The gray dots of pigmented actinic keratoses and Bowen’s disease correspond to melanophages in the papillary dermis. The predominance of the structureless pattern in both lesions indicates the absence of rete ridges (a frequent consequence of heavy UV exposure). The circular arrangement of dots in facial pigmented actinic keratosis is due to the fact that the round openings (infundibula) of hair follicles are non-pigmented and melanophages tend to be arranged around the follicle. The brown dots in pigmented Bowen’s disease correspond to accumulations of melanin in an angiocentric location in the dermal papillae this being the reason red dots in linear array may merge into pigmented dots in the same linear arrangement.

© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
94 Pattern Analysis – Basic Principles
Figure 3.51: Facial pigmented actinic keratosis.
Dermatoscopy, right column. Pigmented actinic keratosis is typically located on the face. Top row: Angulated lines and structureless dominate this actinic keratosis. The structureless pattern is interrupted by the hypopigmented follicular openings. There are some sparse gray dots and prominent scale, which is a good clue to actinic keratosis. Middle row: Angulated lines and gray dots between hypopigmented follicular openings are the patterns of this pigmented actinic keratosis. This pattern can also be seen in melanoma in situ or in lichen pla- nus-like keratosis but the clue of prominent white circles points to the diagnosis of actinic keratosis. Bottom row: Actinic keratosis with a structureless brown pattern and gray dots on dermatoscopy. The clue here is the presence of multiple 4-dot clods (4 white dots arranged in a square). These structures are only seen with polarized dermatoscopy. The sharply demarcated border indicates a collision with solar lentigo.

© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
Pattern Analysis – Basic Principles |
95 |
Figure 3.52: Pigmented Bowen’s disease.
Dermatoscopy, right column. Top row: The most common pattern of pigmented Bowen’s disease is structureless brown. The clue of coiled vessels allows a diagnosis of pigmented Bowen’s disease. Middle row: On dermatoscopy there is more than one pattern (dots and structureless). The dots are gray and brown and peripherally they are, in part, arranged as radial lines (between 9 o’clock and 11 o’clock). Bottom row: On dermatoscopy there is more than one pattern (structureless, dots and small clods). The clue of coiled vessels is suggestive of Bowen’s disease.
© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
96 Pattern Analysis – Basic Principles
Figure 3.53: Dots and coiled vessels arranged in lines in Bowen’s disease.
The dermatoscopic overview on the left shows two patterns (dots and structureless). Brown dots and coiled vessels are arranged in lines in the periphery. The close-up on the right shows a higher magnification of brown dots arranged in lines.
A |
C |
B
Figure 3.54: Pigmented Bowen’s disease induced by human papilloma virus (HPV).
Clinical examination (A) reveals a brown plaque with a scalloped border. Dermatoscopically (B) there are two patterns (structureless and dots). The higher magnification (C) shows brown dots arranged in lines. This clue permits a specific diagnosis.
Pigmented actinic keratosis and pigmented Bowen’s disease
|
Pattern |
Colors |
Clues |
Actinic keratosis, pigmented |
Typical: |
Typical: |
Scale, white circles, 4-dot clod |
(face) |
Structureless, angulated lines, |
Brown (structureless part), Gray |
(4 white dots arranged in a |
|
dots, and occasionally circles |
(dots) |
square), which is visible only |
|
|
|
with polarized dermatoscopy) |
Bowen’s disease, pigmented |
Typical: |
Typical: |
Typical: |
|
Dots (dots arranged in lines |
Brown, occasionally gray. Struc- |
Dots are arranged in lines |
|
may appear as radial lines in |
tureless areas = skin-colored or |
radially at the periphery. Coiled |
|
lower magnification), structure- |
light-brown |
vessels, clustered or arranged in |
|
less |
|
lines, scale. |

© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
Pattern Analysis – Basic Principles |
97 |
3.7 Characteristic features of melanocytic lesions
3.7.1 Melanocytic nevi Clark nevus
The most common acquired nevus is the Clark nevus. While on dermatoscopy it shows remarkably diverse morphology, there are specific features which distinguish the Clark nevus both from other benign nevi on the one hand and melanoma on the other (3.55–3.59). However the range of appearances of Clark nevi does overlap with both superficial congenital nevi and melanoma (especially in situ melanoma) to an extent that differential diagnosis may be quite difficult even with dermatoscopy. This does not mean that a biological zone of overlap actually exists; rather this should be viewed as a limitation of the method.
The reticular pattern usually predominates in the Clark nevus; indeed most often thin reticular lines is the only pattern (3.55). In the growth phase, the reticular pattern may be combined with peripheral dots or clods (3.56). These peripheral structures usually regress as the nevus matures. Clark nevi consisting solely of brown dots or small brown clods are exceptions. Less common again is the combination of the reticular pattern with a structureless zone, nearly always hyperpigmented and located centrally.
In general – as one expects in benign lesions – combinations of patterns are arranged symmetrically in the Clark nevus. The same is not true for arrangements of colors, which may be symmetrical or asymmetrical. As the proliferation of melanocytes in the epidermis is the essential architectural feature of the Clark nevus, the colors are those of melanin in the epidermis: light-brown, dark-brown and black. The commonest arrangements of colors in the Clark nevus are uniform brown pigmentation, and brown peripherally with central hyperpigmentation. This pattern of central hyperpigmentation of a reticular lesion is a clue to the diagnosis of Clark nevus. Pigmentation may also be variegate, or eccentrically hyperpigmented. This pattern of Clark nevi overlaps morphologically with in situ melanoma.
Other features, especially those of melanoma, are usually absent. Occasionally one finds a few gray dots (melanophages in the dermis), erythema (a sign of inflammation) or peripheral radial lines occupying the whole circumference.
Very rarely there may be skin-colored or white reticular lines. It should be noted that grey dots and white lines are also clues to melanoma. In these rare cases it may not be possible to confidently reach a diagnosis of Clark nevus. In general, pattern and color, and the symmetry of their combinations, should be given
greater importance than any single clue to melanoma. The pattern of vessels in Clark nevi is unremarkable: it usually consists of a pattern of dots occasionally interspersed with short vessels, either straight or curved. Distinguishing between a Clark nevus and a “superficial” or a “superficial and deep” congenital nevus is usually simple. Clark nevi are flat clinically while “superficial” or “superficial and deep” congenital nevi are raised. The reticular pattern is predominant in Clark nevus, the clod pattern is usually (but not always) predominant in congenital nevi. Clark nevi are either uniformly pigmented or marked by central or eccentric hyperpigmentation, while small congenital nevi are usually centrally hypopigmented or variegate (see the section on this entity). Confusion arises because most dermatopathologists do not make this distinction, describing both Clark nevi and small congenital nevi as “dysplastic” junctional or compound nevi or simply as a junctional or compound nevus.
Correlation between dermatoscopy and dermatopathology
The 2-dimensional horizontal projection of the 3-dimen- sional rete ridges causes the characteristic reticular pattern on the surface of the skin. The pigmented lines correspond to vertically arranged rete ridges while the hypopigmented center represents the dermal papillae. The brown pigmentation of lines is primarily due to deposits of melanin in basal keratinocytes. Often the melanocytes themselves are not sufficiently pigmented to be visible on dermatoscopy. If they are, they appear as brown dots or clods that correspond to smaller or larger nests of melanocytes at the dermoepidermal junction.
“Superficial” and “superficial and deep” congenital nevi
Like Clark nevi, “superficial” and “superficial and deep” congenital nevi are extremely diverse morphologically, but have specific clues that usually make diagnosis straightforward. Again, it should be remembered that in this context the term “congenital” does not necessarily mean that the nevus was visible at birth. As mentioned in chapter 2, “superficial” and “superficial and deep” congenital nevi have a different architecture to Clark nevi and are usually easy to distinguish from the latter by histopathology.2 As we have described above, this is also true – with certain limitations – of dermatoscopy. While the reticular pattern is predominant in Clark nevus, the clod pattern is predominant in congenital nevi (3.60, 3.61). The clod pattern occurs either alone
2Regrettably, this distinction is not made by many dermatopathologists. Both types of nevi are termed “dysplastic compound nevi” or “compound nevi”.

© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
98 Pattern Analysis – Basic Principles
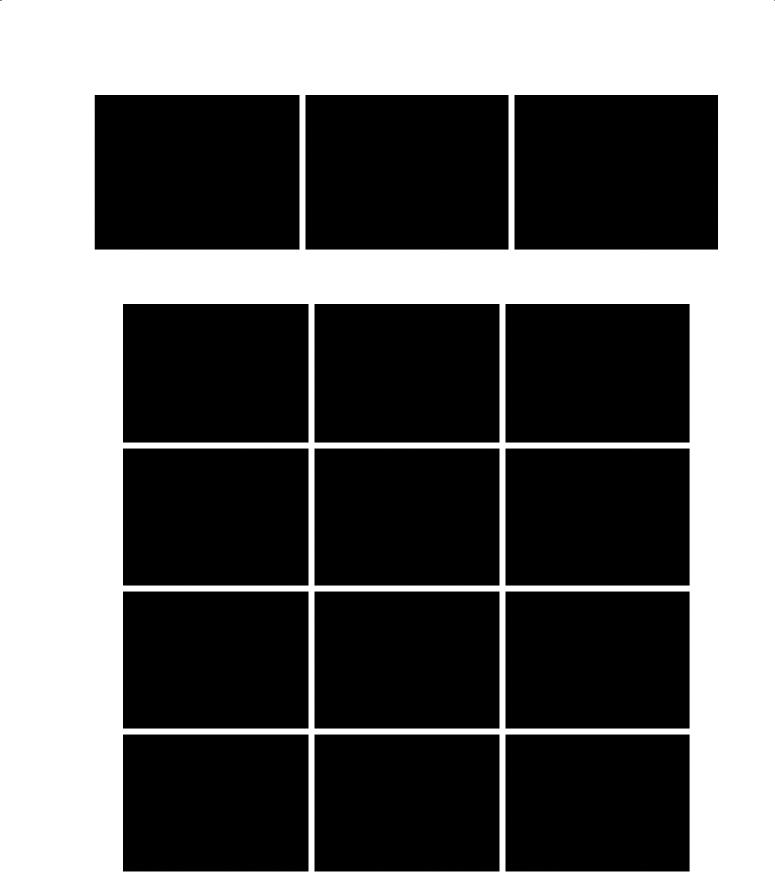
Figure 3.55: Typical Clark nevi.
Dermatoscopy right column. Top row, right: One pattern, reticular, uniformly light-brown. Middle row, right: One pattern, reticular, uniformly light-brown. Bottom row, right: One pattern, reticular, centrally hyperpigmented.
© Dies ist urheberrechtlich geschütztes Material. Bereitgestellt von: TH Mittelhessen Mo, Okt 5th 2020, 09:04
Pattern Analysis – Basic Principles |
99 |
Figure 3.56: Growing Clark nevus.
On dermatoscopy a Clark nevus in the growing phase is typically seen as a symmetrical combination of the reticular pattern in the center and clods peripherally.
Figure 3.57: Clark nevi on the trunk.
Dermatoscopy, right column. Top row: One pattern, reticular lines, light-brown (the hypopigmented structureless area is too small to be interpreted as a pattern). Second row: One pattern, reticular, variegate. Third row: More than one pattern, reticular peripherally, structureless centrally, symmetrically combined, and central hyperpigmentation. Bottom row: One pattern, reticular, eccentric hyperpigmentation.